
Abstract
Purpose
This article examines the extent to which employees worked from home because of the pandemic, focusing on differentials between people with and without disabilities with implications for cancer survivors.
Methods
We use data on COVID-19 from the Current Population Survey over the May 2020 to June 2021 period. We present descriptive statistics and the results from regression and decomposition analysis.
Results
While workers with disabilities were more likely than those without disabilities to be teleworking before the pandemic, they were less likely to be teleworking as a result of the pandemic. Differences in the occupational distribution account for most of this difference. People with disabilities experienced relatively more pandemic-related hardships as well, compared to people without disabilities, including a greater chance of not being able to work due to their employer losing business and more difficulty in accessing medical care.
Conclusions
Many people with disabilities benefit from working from home, and the pandemic has increased employer acceptance of these arrangements, but the potential is limited by the current occupational distribution.
Implications for Cancer Survivors
While the CPS dataset does not have information on cancer survivorship, we use other data to impute that the average likelihood of cancer survivorship is 12.6% among people with disabilities, more than double the 6.1% rate among those without a disability. Hence cancer survivorship is partly picked up by the CPS questions on disability, and our results have implications for cancer survivors, especially because increased opportunities for telework have the potential to help cancer survivors maintain economic stability and avoid financial hardship.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The COVID-19 pandemic caused enormous social and economic hardship around the globe, especially for lower-income and marginalized groups. In the USA, tens of millions of workers lost their jobs in 2020, with disproportionately larger employment losses for people with disabilities, women, Latinx, and Blacks compared to people without disabilities, men, and Whites [1,2,3]. Losses were even greater for people with intersecting marginalized identities. For many others, especially those in white-collar jobs, workplace closures forced employees to telecommute from home, and new studies indicate a substantial increase in work from home during the COVID-19 pandemic compared to before the crisis [4]. This unprecedented increase in working from home may have lasting effects on employers’ acceptance of such arrangements. In particular, telework could become a more common workplace accommodation for persons with disabilities.
By greatly expanding work at home, the crisis creates an ideal opportunity to examine the incidence of home-based work as it relates to disability and cancer survivorship. Home-based work can be particularly valuable for many people with disabilities [5]. It not only can enable job retention, but also may help ensure that pay levels and raises are determined more by actual job performance and qualifications, rather than by stereotypes and workplace cultural dynamics that have been shown to disadvantage workers with disabilities [6]. In some cases, working from home has been considered a reasonable accommodation under the Americans with Disabilities Act (“ADA”) [7], but many employers have been resistant to work from home arrangements along with other ADA requirements [8,9,10].
During the pandemic, people in service and blue-collar occupations were especially hard-hit with job losses—the sectors in which people with disabilities are disproportionately employed. Hence, people with disabilities were probably less likely than people without disabilities to be teleworking and more likely to be laid off. This prediction is consistent with findings in Papanikolaou and Schmidt [11] that sectors in which a larger proportion of workers were not able to work remotely experienced larger declines in employment due to the pandemic.
This study examines the extent to which workers were working from home due to the pandemic, with a focus on whether people with disabilities were more or less likely to be teleworking compared to people without disabilities. It also examines the extent to which COVID-19 restrictions prevented people with disabilities from searching for jobs and obtaining medical services. To determine the implications of these results for cancer survivors, we use a simulation approach to predict the likelihood that someone with a disability is a cancer survivor. To explain the differences in telework incidence between people with and without disabilities, we use a standard regression model as well as a decomposition approach applied to recent data on COVID-19 from the Current Population Survey over the May 2020 to June 2021 period.
Background
The pandemic and telework
The pandemic has brought a surge of scholarly and practical interest in the costs and benefits of working from home. Survey evidence from over 30,000 Americans during the pandemic indicates that 60% of respondents reported an increase in productivity due to work from home arrangements [12]. Combined with other changes during the pandemic, such as reduced stigma around working from home, technological innovations, and investments in human and physical capital that support working from home, these better-than-expected employee experiences with telework may contribute to a four-fold increase in the share of full workdays that are remote, from 5% before the pandemic to 20% after the pandemic [12]. These effects are consistent with some earlier studies, including a controlled randomized experiment by a large Chinese company which found that worker productivity and satisfaction were higher among those who worked at home, and turnover went down [13]. There are also supportive results from teleworkers in the US federal government [14]. In addition, firms with greater telework flexibility had higher stock returns during the pandemic [15]. The Chinese company study did, however, identify a downside: employees who teleworked were less likely to receive promotions, suggesting that remote workers are more likely to be “out of sight, out of mind” [13]. It is important to examine different types of workers, as other studies have found negative productivity effects during the pandemic, including a study of 10,000 IT workers at a large Asian company which found that hours worked increased as a result of working from home during the pandemic, largely due to the increased time costs of communication and coordination, and average productivity declined, especially for employees with children [16]. These findings on productivity declines for workers (predominantly women) with children are supported elsewhere [17,18,19].
People with disabilities experienced disproportionately greater job losses during the pandemic compared to people without disabilities [2]. It also took longer for them to regain employment in the latter part of 2020. A substantial portion of the increased employment gap between people with and without disabilities is explained by how the pandemic differentially affected occupations and industries. Among those who are employed, workers with disabilities are underrepresented in white-collar jobs and overrepresented in service and blue-collar jobs [5, 20]. While these types of jobs are less amenable to telework, pre-pandemic data show that people with disabilities were in fact about 20% more likely to work at home than otherwise-similar workers without disabilities [5]. This differential points to the benefits that working from home can provide to persons with mobility impairments or other conditions that make it difficult to work a regular schedule at the employer’s location. This may also reflect the reluctance of employers to hire people with disabilities into jobs with face-to-face contact with co-workers or customers, due to stigma, bias, and discrimination on the basis of disability, or other reasons [21].
Cancer and employment
Prior to the passage of the ADA Amendments Act (“ADAAA”) in 2008 [22], federal courts were divided on whether cancer survivors had a legally recognized disability under the ADA. The ADAAA explicitly rejected a “narrow, demanding standard for qualifying as disabled” in favor of a “broad scope of protection,” which has significantly improved the ability of cancer survivors to prove disability status [23]. Many of the hundreds of thousands of Americans who are diagnosed with cancer each year and who seek reasonable accommodations at work may be legally entitled to those accommodations under the ADA [23, 24]. As of 2019, there were 16.9 million cancer survivors in the USA, and 36% of those survivors were of working age (20–64), making the question of employer accommodations a highly relevant issue for cancer survivors [25].
Not only do individuals going through cancer treatments experience substantial disruptions to their physical and mental health that may necessitate reasonable accommodations, but also survivors often have long-term health impairments. Many survivors of childhood cancer have functional or cognitive disabilities that can impact their schooling and employment [25]. Furthermore, cancer can reoccur, and some survivors may need ongoing or periodic accommodations from employers. Cancer can have a large negative impact on employment and economic security [26, 27]. Recent evidence suggests that hardships for cancer survivors and their caregivers have increased during the pandemic, particularly with the stress and confusion of navigating a complicated set of laws and policies around workplace accommodations and health insurance coverage [28].
A 2015 US study found that the probability of a cancer patient being employed dropped by almost 10 percentage points, and hours worked declined by up to 200 hours, in the first year after diagnosis [29]. Annual labor market earnings dropped almost 40% within 2 years after diagnosis and remained low, whereas total family income declined by 20% [29]. Another longitudinal study of working-age female early-stage breast cancer survivors in the USA found that fatigued patients, African American patients, and publicly insured or uninsured patients with cancer were more likely to experience diminished employment after 2 years of follow-up [30]. For people undergoing chemotherapy, the unavailability of employer accommodations during treatment contributes to the negative, and often illegal discriminatory, effects of chemotherapy on work [31]. Patients who lack accommodations may be unable to work during treatment, and if they do not have sick leave, they may be replaced if they take time off [26, 32]. Low-income workers and people of color are less likely to receive workplace accommodations [9, 33].
“Financial toxicity” may result from decreased earnings and increased spending after a cancer diagnosis, leading to increased symptoms and emotional distress and decreased quality of life and treatment adherence [34]. A 2011 study found that unsupportive work environments — including perceived discrimination, manual work, low income, older age, lower education levels, and being female — were barriers among survivors to returning to work [35]. Among breast cancer survivors, Black, Asian, and Latinx survivors were less likely to be employed 4 months after treatment completion [33].
Disability and home-based work
Relatively little is known about the incidence or effects of home-based work for workers with disabilities. Although many people with disabilities identify work flexibility as important [36], many managers and employees express concerns with telework arrangements for workers with disabilities [37]. Low wage, part-time, contingent, and gig jobs — more often held by workers with disabilities — generally do not provide paid sick leave, family and medical leave, and other benefits enjoyed by people without disabilities in standard jobs [38]. People with disabilities have, on average, higher numbers of doctor’s office and hospital visits than those without disabilities [39]. Working in jobs without a safety net of paid sick or medical leave or options for teleworking puts people with disabilities at higher risk for loss of jobs, wages, independence, and economic self-sufficiency.
The restructuring of many jobs during the pandemic may ultimately benefit people with disabilities by making employers more willing to accommodate the need for home-based work [5]. People with disabilities were more likely to be working from home before the pandemic [5], but as noted, they are generally less likely to be in occupations that are amenable to telework [5], meaning that they may be left behind in any rapid expansion of telework such as occurred during the pandemic.
This article aims to contribute to gaps in the literature by examining the expansion of telework triggered by the COVID-19 pandemic. We focus on the importance and effects of home-based work for people with disabilities who can benefit from flexible scheduling and individualized accommodations. Due to their underrepresentation in occupations amenable to telework, we hypothesize that (a) the increase in working from home during the pandemic was lower among workers with disabilities; (b) most of the telework gap between people with and without disabilities will be explained by the occupational distribution; and (c) people with disabilities had more difficulty looking for new jobs and accessing medical care compared to people without disabilities. This research will provide new evidence on the extent to which the occupational distribution explains telecommuting differences between individuals with and without disabilities, and how cancer survivors are likely to have weathered the storm of the pandemic compared to people who have not had cancer.
Data and methodology
In this study, employment and telework measures are constructed using data from the Current Population Survey (“CPS”), a monthly survey collected by the Bureau of Labor Statistics, with a sample of about 1,800,000 individuals per year. It provides data on demographic characteristics as well as measures of disability based on a six-question set asked since 2008: (1) “Is this person deaf or does he/she have serious difficulty hearing?”; (2) “Is this person blind or does he/she have serious difficulty seeing even when wearing glasses?”; (3) “Because of a physical, mental, or emotional condition, does this person have serious difficulty concentrating, remembering, or making decisions?”; (4) “Does this person have serious difficulty walking or climbing stairs?”; (5) “Does this person have difficulty dressing or bathing?”; (6) “Because of a physical, mental, or emotional condition, does this person have difficulty doing errands alone such as visiting a doctor’s office or shopping?”. Respondents may choose more than one category, so the categories are not mutually exclusive.
The six disability questions thus identify hearing, vision, cognitive, and mobility impairments and difficulty with self-care or going outside alone. In May 2020, the CPS started asking a special set of five questions each month about whether people were working at home or not working at all, due to COVID-19. These questions ask whether or not in the past 4 weeks at any time the respondent: (1) worked from home for pay because of the pandemic; (2) was unable to work because their employer closed or lost business; (3) received pay from their employer for hours not worked; (4) was prevented from looking for work due to the pandemic; and (5) was prevented from getting healthcare due to the pandemic [40]. An important note is that these questions specify that the outcome had to occur because of the pandemic. For question 1, this means that pre-existing home-based work is not measured, so these numbers should not be taken as a measure of the total amount of home-based work during the pandemic.
While the CPS data do not measure cancer survivorship, we take advantage of another representative survey to impute cancer survivorship for this sample based on their demographic characteristics and responses to the six CPS disability questions. The Behavioral Risk Factor Surveillance System (“BRFSS”), coordinated by the Centers for Diseases Control (“CDC”), surveys people in each state about their health and health behaviors (data available at https://www.cdc.gov/brfss/index.html). The 2019 data used here include 418,268 observations on adults ages 18 or older. Since 2014 the surveys have included the six census measures used by the CPS. To measure cancer survivorship, we use two questions from the BRFSS that ask whether the respondent had ever been told s/he had skin cancer or any other type of cancer (the question wordings are found in the Appendix). We use a probit model to predict cancer survivorship with a full set of interactions among the six CPS disability measures, plus gender, age, race/ethnicity, and employment status (i.e., whether the respondent is employed, self-employed, or reports being unable to work); the BRFSS descriptive statistics are in Appendix Table 6, and the results of the probit regression are found in Appendix Table 7. The coefficients were then used in the CPS sample to predict the likelihood of being a cancer survivor. Appendix Table 8 reports sample means for all variables from the CPS, in total and disaggregated by disability status.
The current analysis focuses on the intersection of telework with disability, considering the degree to which people with disabilities were especially likely to be teleworking due to the pandemic, and how this changed over time. The data are first used to construct descriptive statistics on telework by disability status. These statistics are then broken down by occupations and industries. We then analyze the relationship between disability and telework in two ways. First, we run linear probability regressions to predict the likelihood of telework, first with disability status only, then controlling for detailed occupations, and then controlling for detailed industries and demographic characteristics (i.e., gender, age, race/ethnicity, education, and number of own children under age 18). We repeat these regressions using the six measures of disability as predictors.
Finally, we conduct a decomposition analysis to examine the extent to which the differences in telework rates between those with and without a disability are explained by differences in observed characteristics or remain unexplained. The decomposition, which is based on logit regressions for telework status, follows the precedent set by Fairlie [41, 42] and is a variation of the common Oaxaca-Blinder decomposition first developed to explain wage gaps [43, 44]. The explained gap is the portion of the gap attributed to disability differences in demographic, occupation, and industry variables; the residual gap is the portion attributed to disability differences in market returns to those characteristics.
To best approximate the baseline structure of telework determinants that would exist in the absence of discrimination or other differential treatment based on disability, we use the coefficients from pooled regressions as suggested by Neumark [45] and Oaxaca and Ransom [46]. The residual (unexplained) telework gap is the difference between actual telework rates and predicted telework rates. The decomposition presents the estimated contribution attributable to differences in the mean levels of the observable characteristics (i.e., occupation, industry, and demographic characteristics). Note that it is possible for the explained gap to exceed 100%, which would happen in the case when the gap would flip to showing the opposite relationship (e.g., a higher rather than lower rate among people with disabilities) if the average characteristics were the same across people with and without disabilities.
Results
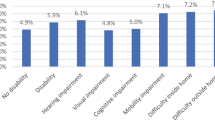
We find that 14.5 million (7.4%) of working-age people during the sample period had disabilities, as represented by a “yes” answer to one or more of the disability questions. As shown in Table 1, the most common type of disability is a mobility impairment, reported by 3.7% of this sample, followed by 3.0% who reported a cognitive impairment, and 2.6% who reported a health condition that makes it difficult to go outside alone. These disabilities likely overlap, as a person may have more than one condition. The coefficients will show the average effect of a disability type when controlling for other disability types. In our analysis, we also test a specification with mutually exclusive disability categories for those reporting one condition and a separate variable for combining those reporting multiple conditions.
Using the imputation process from BRFSS as described above, we estimate that the average probability of being a cancer survivor in our sample is 6.5%, representing 12.9 million working-age people. The third column of Table 1 shows that the mean likelihood of cancer survivorship is 12.6% among people identified with disabilities by the CPS measures, which is more than double the 6.1% rate among those not identified as having a disability. Since this is an imputed probability, it does not clearly distinguish those who are and are not cancer survivors, but there is no obvious upward or downward bias in the overall mean likelihood. Recognizing the limitations of this imputed variable, it is nonetheless helpful in showing the relationship between cancer survivorship and the CPS disability variables and supporting that our CPS results are relevant to cancer survivors.
While not a primary focus of this article, it is important to note that people with disabilities are less likely than non-disabled people to be employed. In the current data, we find that only 29.8% of working-age people with disabilities were employed in the average month, from May 2020 to June 2021, compared to 72.6% of people without disabilities. Past research has tied lower employment of people with disabilities to worker characteristics such as education, disincentives from disability income programs, and employer reluctance to hire people with disabilities that may reflect prejudice and discrimination [47, 48].
As predicted, among employed people, relatively more of those without a disability reported that they were engaged in telework due to the pandemic compared to people with a disability. Among employed people over the whole period, Table 2 shows that an average of 19.4% of people with disabilities did pandemic-related telework, which is significantly lower than the 23.6% figure for people without disabilities. Among people with disabilities, the rate was especially low for people with visual impairments (17.2%) and highest for people with cognitive impairments (20.8%).
The telework figures vary over time, decreasing as vaccines became more available and people returned to on-site work. As shown in panel A of Fig. 1, in May 2020, when the question about telework was first included in the CPS, 35.8% of people without a disability were teleworking, compared to 25.7% of people with a disability. This gap slowly narrowed as the pandemic continued but did not disappear entirely. By June 2021, 14.5% of people without a disability were engaged in telework, compared to 12.7% of people without a disability. Thus, telework incidence declined over the course of the pandemic, but it declined relatively more for people without disabilities.

Percentage of workers engaged in telework by disability status and gender
A similar pattern holds for women compared to men in panel B. Throughout the pandemic, relatively more women than men reported working from home. The most likely explanation for this gender differential is women’s relatively greater caregiving responsibilities at home as schools and daycare centers closed, and their paid and unpaid work obligations overlapped. As the pandemic wore on, however, the percentage of workers who engaged in telework declined for both women and men, and the relative decline was larger for women than men. Finally, panel C reports patterns of telework when we interact disability status with gender, taking an intersectional viewpoint [9]. Overall, throughout the May 2020 to June 2021 period, women without disabilities were most likely to engage in telework and men with disabilities the least likely. The gap between these two groups amounted to almost 20 percentage points in May 2020, but then it steadily declined over time. Interestingly, women with a disability had comparable rates of telework as men without a disability. This similarity reflects the combined but competing forces of women teleworking more than men due to increased caregiving responsibilities but people with disabilities teleworking relatively less due to the pandemic (in part because they had a higher likelihood pre-pandemic of already working from home).
While the focus of this article is on telework, Table 2 also presents summary results for the four other CPS pandemic outcomes. Consistent with prior data on higher layoff rates among people with disabilities [49], the reported rate of inability to work due to employer cutbacks is 3.5 percentage points higher for people with disabilities than for those without disabilities. Among those who were unable to work, the incidence of people with disabilities being paid for the time they were not working was 3.8 points lower than those without disabilities. Among those who were not in the labor force, the incidence of people with disabilities reporting that the pandemic prevented them from searching for work was 6.1 percentage points lower, reflecting generally lower labor force participation among people with disabilities. Finally, the percent of people with disabilities reporting that someone in their household needed medical care but did not get it due to the pandemic was 5.6 points greater than among those without disabilities.
Turning back to telework, Table 3 presents a breakdown by major occupation and industry. As expected, people who worked in white-collar occupations reported a higher incidence of telework compared to other occupations. Table 3 shows the highest rate of telework in management, business, and financial occupations (i.e., 42.5% for workers without disabilities and 36.4% for workers with disabilities), followed by professional occupations and office and administrative support. In comparison, relatively few people worked from home in blue-collar and low-wage occupations where workers with disabilities are traditionally concentrated, including production, transportation, and service jobs. These results are consistent with prior findings that in May to December 2020, not surprisingly, rates of telework were substantially higher in white-collar occupations considered to be suitable for telework compared to occupations not suitable for telework according to Occupational Information Network (O*NET) measures of occupational skill requirements and how the work is conducted [4].
A pattern exists across industries, with the highest rates of telework in industries considered to have mostly white-collar jobs (e.g., information services, financial activities, professional services, and public administration). In contrast, the lowest rates of telework are found in industries considered to be blue-collar (e.g., transportation, construction, agriculture) and/or low pay (e.g., leisure and hospitality). Interestingly, the incidence of telework is higher among people without disabilities compared to people with disabilities in almost every occupation and industry, with the biggest exception being public administration. In this case, 34.7% of people without disabilities reported working from home compared to 38.8% of people with disabilities, most likely reflecting a greater likelihood of the public sector complying with the ADA mandate to provide reasonable accommodations.
Predictions of telework when controlling for other factors are presented in Table 4. Column 1 shows that people with disabilities are 4.2 percentage points less likely than people without disabilities to telework due to the pandemic, controlling only for month of the survey. This highly significant gap decreases to a non-significant 0.8-point difference when controlling for detailed occupation, indicating that the lower overall rate of telework among people with disabilities is largely due to their higher likelihood of being in blue-collar and service occupations that are not as amenable to telework. The coefficient remains small in magnitude but becomes positive and statistically significant in column 3 when further controlling for detailed industry and demographic characteristics. The higher likelihood of telework among people with disabilities when controlling for detailed characteristics is consistent with pre-pandemic data on the higher likelihood of home-based work among people with disabilities [5].
Column 3 also shows that telework is higher among women than among men, and especially high among those with college and graduate degrees. Moreover, the likelihood of telework drops with age. Given that the risk of disabilities often increases with age, it is not surprising that adding age as a control variable affects the disability coefficient.
Interestingly, the likelihood of telework drops with part-time status as well as self-employment status. One might reasonably expect that part-time workers are less likely to have non-pecuniary work benefits such as the ability to work from home. The most likely explanation for the negative coefficient for self-employment is that self-employed people were already more likely to work from home before the pandemic and thus had less potential for expanded telework during the pandemic. In other words, self-employed people who could work at home pre-pandemic were already engaged in telework, so the increase was more limited for self-employed individuals during the pandemic.
Differences across disability types are analyzed in columns 4 to 6. As in column 1, the regression in column 4 includes only a control variable for survey month. In this case, five of the six measures of disability are negatively associated with the likelihood of teleworking, and four of those are statistically significant. The disability with the largest coefficient is visual impairment.
These results indicate that individuals with most types of disabilities, and especially those with visual impairments, were less likely to telework during the pandemic than individuals without disabilities. In robustness checks using the alternative construction of the disability dummy variables with mutually exclusive categories (not reported here but available), our regression results are substantively the same as those reported in Table 4. After we control for occupation, having a visual impairment is still negatively associated with the likelihood of engaging in telework, and having a cognitive impairment raises the likelihood of telework during the pandemic. However, the coefficients for the other types of disabilities become smaller in magnitude and statistically insignificant, indicating that for people with those types of disabilities, the lower rate of telework is largely due to their higher likelihood of being in occupations that are not amenable to telework. In the final column, when we control for the full set of demographic characteristics as well as occupation and industry, the only type of disability that has a significant coefficient is cognitive impairment.
For the most part then, these results suggest that after controlling for occupation, industry, and other characteristics, having a disability has fairly small predictive power in determining the likelihood of telework during the pandemic; what matters more is being a woman, having higher levels of education, being younger, and working in an occupation or industry that is amenable to telework. These results are similar to findings for a sample of lawyers before the pandemic regarding gender and age and who is more likely to request an accommodation [9]. The only exception is people with a cognitive impairment, who were about 3 percent more likely to work remotely during the pandemic compared to people without any impairment.
Recall from Table 1 that cognitive impairments are the second largest source of disability, and about 11% of people with cognitive impairments are cancer survivors. Adults who had childhood cancer are particularly at risk of having a cognitive impairment. Earlier research indicates that work from home has unique benefits for individuals with cognitive health issues who may value being away from a stressful environment and who may need to take unscheduled breaks [5, 50]. During the pandemic such features of the work environment were becoming more commonplace, thus making it less surprising that the likelihood of telework rose for individuals with cognitive impairments even after controlling for occupation, industry, and other characteristics.
We assess the contributions of specific variables to the difference in telework between people with and without disabilities using the decomposition approach, with results presented in Table 5. There, 121.6% of the 4.2 point disability gap in telework is statistically “explained” by differences in mean values of the predictors. The fact that the figure is over 100% indicates that if the mean values were identical on all predictors between the two groups, the gap would be more than erased, and people with disabilities would be predicted to have a slightly higher likelihood of telework than people without disabilities. This higher likelihood is supported by the statistical significance of the “unexplained” component and is consistent with the positive coefficient on disability in column 3 of Table 4. The biggest contributor to the overall disability gap is differences in the occupational distribution, statistically accounting for 51.3% of the raw gap. The other major contributors are education (38.2%), industry (10.8%), and part-time employment (10.2%), with little role played by other demographic predictors.
The results are broadly consistent when decompositions are done separately for each type of disability (not presented here but available), with the bulk of the disability telework gap being explained by different mean levels of the predictors. Occupation continues to be the largest contributor to the telework gap among people with hearing impairments, cognitive impairments, and difficulty going outside alone, while education is the largest contributor among those with vision impairments, mobility impairments, and difficulty dressing or bathing. Consistent with the positive significant coefficient for mental disability in the regression in column 6 of Table 4, there is a significant “unexplained” component of the telework gap among people with mental impairments after controlling for the other predictors. This may be due to features of telework not specific to occupations, such as the need for a less risky and stressful environment and more flexibility for work breaks, that can be particularly important for people with mental disabilities. This result is relevant as many people with chronic health conditions (cancer included) tend to report cognitive conditions or generally report poor mental health.
Conclusion
Many workers with disabilities have conditions that make it difficult and risky to work on site during a pandemic, including cancer survivors with compromised immune systems. Results from this analysis, the first to examine the incidence of telework among people with disabilities during the COVID-19 pandemic, indicate that people with disabilities were less likely to work from home due to the pandemic compared to people without disabilities. During the May 2020 to June 2021 period, 19.4% of workers with disabilities engaged in pandemic-related telework, compared to 23.6% of employees without disabilities. Ironically, this outcome is the opposite of pre-pandemic patterns when workers with disabilities were more likely to work from home [5].
People with disabilities experienced relatively more pandemic-related hardships as well, compared to people without disabilities, including a greater chance of not being able to work due to their employer losing business, a lower likelihood of receiving pay if they were unable to work, and more difficulty in accessing medical care for themselves or a household member. These results have practical relevance for cancer survivors, given our estimate of a 12.6% likelihood that someone with a disability is a cancer survivor.
Results from regression models indicate that the lower overall rate of telework among people with disabilities is primarily due to their greater likelihood of working in blue-collar and service occupations that are not as conducive to telework. Overall, more than half (54%) of the gap in telework between people with and without disabilities is explained by differences in the occupational distribution. Other predictors of telework include gender (being a woman), education (having a bachelor’s or graduate degree), and age (being younger than 50). Closer consideration of specific types of disability indicates that people with cognitive disabilities were an exception and, in fact, more likely to engage in telework during the pandemic, possibly because key aspects of telework can be valuable to people with cognitive impairments, such as a less stressful environment and more flexibility for work breaks.
These results shine new light on the importance of longer-term structural changes to the occupational distribution to ensure that people with disabilities are less concentrated in blue-collar and essential service jobs that tend to have lower pay and less job security. The pandemic has brought greater employer acceptance of working from home. However, if persons with disabilities are clustered in jobs that are less conducive to telework, it will be more difficult to require an employer to provide this accommodation to workers with disabilities. At the same time, even if they are allowed to work from home, it is important that teleworkers do not find themselves “out of sight, out of mind” and that they receive fair pay and equal opportunities for promotions. These concerns are particularly important for people with disabilities, many of whom value and require working at home, and who were generally more likely to be in telework arrangements before the pandemic.
There are more than 17 million cancer survivors in the USA and close to 40% of those survivors are of working age (20–64). Increased opportunities for telework have the potential to help many cancer survivors maintain economic stability and avoid financial toxicity. Having the option to work from home can be critically important for cancer survivors, both those undergoing treatment and those with more permanent health impairments. Given the paucity of research on work from home arrangements among people with disabilities, our findings constitute a meaningful increase in knowledge of the incidence of home-based work among workers with disabilities and the implications for cancer survivors. Continuing technological developments are rapidly reshaping work and increasing the feasibility of working remotely in many occupations. Given the growth and potential benefits of telework, this is a valuable and important area for further research.
Data availability
The CPS data are available from the Census Bureau, and the BRFSS data are available from the Centers for Disease Control.
Code availability
The analysis was conducted using StataMP 16 and the Stata do files are available from the corresponding author on reasonable request.
References
Ansell R, Mullins JP. COVID-19 ends longest employment recovery and expansion in CES history, causing unprecedented job losses in 2020. Mon Labor Rev. U.S. Bureau of Labor Statistics. 2021 https://doi.org/10.21916/mlr.2021.13
Schur L, Rodgers Y, Kruse D. COVID-19 and employment losses for workers with disabilities: an intersectional approach. Soc Sci Res Netw. 2021. https://doi.org/10.2139/ssrn.3788319.
Smith SM, Edwards R, Duong HC. Unemployment rises in 2020, as the country battles the COVID-19 pandemic. Mon Labor Rev. U.S. Bureau of Labor Statistics. 2021; https://doi.org/10.21916/mlr.2021.12
Dey M, Frazis H, Piccone DS Jr, Loewenstein MA. Teleworking and lost work during the pandemic: new evidence from the CPS. Monthly Labor Review. U.S. Bureau of Labor Statistics. 2021; https://doi.org/10.21916/mlr.2021.15
Schur L, Ameri M, Kruse D. Telework after COVID: a ‘silver lining’ for workers with disabilities? J Occup Rehabil. 2020;30:521–36.
Schur L, Kruse D, Blanck P. People with disabilities: sidelined or mainstreamed? Cambridge University Press; 2013.
U.S. EEOC. Work at home/telework as a reasonable accommodation. EEOC-NVTA-2003–1. 2003. https://www.eeoc.gov/laws/guidance/work-hometelework-reasonable-accommodation. Accessed 30 July 2021.
Kaye HS, Jans LH, Jones EC. Why don’t employers hire and retain workers with disabilities? J Occup Rehabil. 2011;21(4):526–36.
Blanck P, Hyseni F, Altunkol WF. Diversity and inclusion in the legal profession: preliminary findings on workplace accommodations from a national study of lawyers with disabilities. J Occup Rehabil. 2020;30:537–64.
Schur L, Nishii L, Adya M, Kruse D, Bruyère SM, Blanck P. Accommodating employees with and without disabilities. Hum Resour Manag. 2014;53(4):593–621.
Papanikolaou D, Schmidt LDW. Working remotely and the supply-side impact of Covid-19. No. w27330. National Bureau of Economic Research. 2020; http://www.nber.org/papers/w27330
Barrero JM, Bloom N, Steven JD. Why working from home will stick. No. w28731. National Bureau of Economic Research. 2021; http://www.nber.org/papers/w28731
Bloom N, Liang J, Roberts J, Ying ZJ. Does working from home work? Evidence from a Chinese experiment. The Q J Econ. 2015;130(1):165–218.
Nuwer R. No workplace like home. Sci Am Mind. 2016;27(5):38–43.
Favilukis JY, Lin X, Sharifkhani A, Zhao X. Labor force telework flexibility and asset prices: evidence from the COVID-19 pandemic. Soc Sci Res Netw. 2020. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3693239.
Gibbs M, Mengel F, Siemroth C. Work from home & productivity: evidence from personnel & analytics data on IT professionals. UChicago, Becker Friedman Institute for Economics Working Paper. 2021 May 6(2021–56). https://ssrn.com/abstract=3843197.
Du M. Locked-in at home: female analysts’ attention at work during the COVID-19 pandemic. 2020. https://ssrn.com/abstract=3741395.
Barber BM, Jiang W, Morse A, Puri M, Tookes H, Werner IM. What explains differences in finance research productivity during the pandemic? J Finance. 2021;76(4):1655–97.
Alon T, Coskun S, Doepke M, Koll D, Tertilt M. From Mancession to shecession: women’s employment in regular and pandemic recessions. National Bureau of Economic Research. 2021. https://www.nber.org/papers/w28632.
Bureau of Labor Statistics. Persons with a disability: labor force characteristics—2019. USDL-20–0339. U.S. Bureau of Labor Statistics. 2020.
Blanck P, Hyseni F, Altunkol WF. Diversity and inclusion in the legal profession: discrimination and bias reported in a national study of lawyers with disabilities and lawyers who identify as LGBTQ+. Am J Law & Med. 2021;46(4):21–63.
ADA Amendments Act of 2008, U.S. equal employment opportunity Commission, eeoc.gov.
Hoffman B. Between a disability and a hard place: the cancer survivors’ Catch-22 of proving disability status under the Americans with Disabilities Act. Md L Rev. 2000;59(2):352–439.
Hoffman B. The law of intended consequences: did the Americans with Disabilities Act Amendments Act make it easier for cancer survivors to prove disability status? NYU Ann Surv Am L. 2012;68:843.
American Cancer Society. Cancer treatment & survivorship facts & figures 2019–2021. Atlanta: American Cancer Society; 2019.
Blinder VS, Gany FM. Impact of cancer on employment. J Clin Oncol. 2020;38(4):302.
Moran JR, Short PF, Hollenbeak CS. Long-term employment effects of surviving cancer. J Health Econ. 2011;30(3):505–14.
Bryant M, Knox S. Cancer in the time of COVID. Health Lawyer. 2021;33(3):39–49.
Zajacova A, Dowd JB, Schoeni RF, Wallace RB. Employment and income losses among cancer survivors: estimates from a national longitudinal survey of American families. Cancer. 2015;121(24):4425–32.
Ekenga CC, Perez M, Margenthaler JA, Jeffe DB. Early-stage breast cancer and employment participation after 2 years of follow-up: a comparison with age-matched controls. Cancer. 2018;124:2026–35.
Blanck P. Disability Inclusive Employment, Cancer Survivorship, and the American with Disabilities Act. J Cancer Survivorship. 2021.
Mujahid MS, Janz NK, Hawley ST, Griggs JJ, Hamilton AS, Katz SJ. The impact of sociodemographic, treatment, and work support on missed work after breast cancer diagnosis. Breast Cancer Res Treat. 2010;119(1):213–20.
Blinder V, Eberle C, Patil S, Gany FM, Bradley CJ. Women with breast cancer who work for accommodating employers more likely to retain jobs after treatment. Health Aff. 2017;36(2):274–81.
Fenn KM, Evans SB, McCorkle R, DiGiovanna MP, Pusztai L, Sanft T, et al. Impact of financial burden of cancer on survivors’ quality of life. J Oncol Pract. 2014;10(5):332–8.
Mehnert A. Employment and work-related issues in cancer survivors. Crit Rev Oncol Hematol. 2011;77:109–30.
Heisey A. Telework: exploring the link between disability, work/family balance, and flexibility. In Information Resources Management Association, editor. Remote Work and Collaboration: Breakthroughs in Research and Practice. IGI Global; 2017 322–345.
Bosua R, Gloet M. Access to flexible work arrangements for people with disabilities: an Australian study. In: Blount Y, Gloet M, editors. Anywhere Working and the Future of Work. IGI Global; 2017 134–161.
Harpur P, Blanck P. Gig workers with disabilities: opportunities, challenges, and regulatory response. J Occup Rehabil. 2020;30(4):511–20.
Kruse D. Demographic, income, and health care characteristics, 1993. Mon Lab Rev. 1998;121:13.
Current Population Survey. COVID-19 items extract files. Technical Documentation. 2020 https://www2.census.gov/programs-surveys/cps/techdocs/Covid19_TechDoc.pdf
Fairlie RW. The absence of the African-American owned business: an analysis of the dynamics of self-employment. J Labor Econ. 1999;17(1):80–108.
Fairlie RW. An extension of the Blinder–Oaxaca decomposition technique to logit and probit models. Center Discussion Paper. No. 873. Yale University. Economic Growth Center. New Haven, CT. 2003.
Oaxaca R. Male–female differentials in urban labor markets. Int Econ Rev. 1973;14(3):693–709.
Blinder A. Wage discrimination: reduced form and structural estimates. J Hum Resour. 1973;8(4):436–55.
Neumark D. Employers’ discriminatory behavior and the estimation of wage discrimination. J Hum Resour. 1988;23(3):279–95.
Oaxaca RL, Ransom MR. On discrimination and the decomposition of wage differentials. J Econ. 1994;61(1):5–21.
Ameri M, Schur L, Adya M, Bentley S, McKay P, Kruse D. The disability employment puzzle: a field experiment on employer hiring behavior. Ind Labor Relat Rev. 2018;71:329–64.
Schur L, Han K, Kim A, Ameri M, Blanck P, Kruse D. Disability at work: a look back and forward. J Occup Rehabil. 2017;27(4):482–97.
Mitra S, Kruse D. Are workers with disabilities more likely to be displaced? Int J Hum Resour Manag. 2016;27(14):1550–79.
Reynolds BW. The mental health benefits of remote and flexible work. In: Mental Health America. 2020. https://www.mhanational.org/blog/mental-health-benefits-remote-and-flexible-work. Accessed 30 July 2021.
Funding
This line of study was supported in part by a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) for the Rehabilitation Research & Training on Employment Policy: Center for Disability-Inclusive Employment Policy Research Grant #90RTEM0006-01–00 and by the RRTC on Employer Practices Leading to Successful Employment Outcomes Among People with Disabilities, Douglas Kruse PI, Grant #90RTEM0008-01-00. The views provided herein do not necessarily reflect the official policies of NIDILRR nor do they imply endorsement by the Federal Government.
Author information
Authors and Affiliations
Contributions
All authors collaborated in conceiving the study’s idea, aims, and design. DK led the data extraction and data analysis process, with assistance from SP. LS and YR were responsible for writing the initial draft, with key input from DK to shape the direction and conclusions of the study. All authors assisted with editing the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix: Imputing cancer survivorship
Appendix: Imputing cancer survivorship
The Current Population Survey (CPS) has six disability questions, but no question related to cancer. To establish the relevance of our findings to cancer survivorship, we impute the likelihood of being a cancer survivor in the CPS sample by using data from the Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS is a series of representative surveys done by each state and coordinated by the Centers for Disease Control, with a total sample of over 400,000 adult respondents per year. The two cancer survivorship questions in BRFSS are based on the following stem: “Has a doctor, nurse, or other health professional ever told you that you had any of the following?” with the specific questions listing “Skin cancer?” “Any other type of cancer?” The percentage answering “yes” to either of these questions, weighted using BRFSS weights, is 12.3%. Restricted to working-aged people (18–64), the percentage is 6.9%.
We predict cancer survivorship using a probit equation with the full set of six interacted CPS disability questions plus gender, age, race/ethnicity, and employment status (employed, self-employed, and unable to work) as predictors. Experiments with other predictors, including interactions of the disability and demographic variables, produced similar results. The regression uses BRFSS weights with Stata’s “pweight” option designed for survey data. The descriptive statistics are in Appendix Table 6 below, followed by the probit results in Appendix Table 7. The Wald chi-squared statistic (84 degrees of freedom) is 12208.88, and the pseudo-R squared is 0.193. These coefficients were then used with the same predictors in the CPS database to estimate the probability of cancer survivorship for each individual. The mean predicted probability in the CPS database (using CPS weights) is 0.118 among all adults ages 18 or older, with a median of 0.063, minimum of 0.001, and maximum of 0.732. Among those age 18–64, the mean is 0.065 with a median of 0.039, minimum of 0.001, and maximum of 0.599.
Table
Table
Table
Rights and permissions
About this article

Cite this article
Kruse, D., Park, S.R., van der Meulen Rodgers, Y. et al. Disability and remote work during the pandemic with implications for cancer survivors. J Cancer Surviv 16, 183–199 (2022). https://doi.org/10.1007/s11764-021-01146-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-021-01146-z