
Abstract
The next generation of climate-driven, disease prediction models will most likely require a mechanistically based, dynamical framework that parameterizes key processes at a variety of locations. Over the next two decades, consensus climate predictions make it possible to produce forecasts for a number of important infectious diseases that are largely independent of the uncertainty of longer-term emissions scenarios. In particular, the role of climate in the modulation of seasonal disease transmission needs to be unravelled from the complex dynamics resulting from the interaction of transmission with herd immunity and intervention measures that depend upon previous burdens of infection. Progress is also needed to solve the mismatch between climate projections and disease projections at the scale of public health interventions. In the time horizon of seasons to years, early warning systems should benefit from current developments on multi-model ensemble climate prediction systems, particularly in areas where high skill levels of climate models coincide with regions where large epidemics take place. A better understanding of the role of climate extremes on infectious diseases is urgently needed.
Similar content being viewed by others


1 Introduction
Human-induced climate disruption is already having a profound effect on many biological systems. Of particular concern is the impact of climate change on the spread and prevalence of parasitic and zoonotic disease agents. Climate change might lead to changes in the geographical range of some parasites and pathogens responsible for serious diseases; equally important and more predictable are changes in the rates of transmission of pathogens where they currently exist. There is also evidence that climate change might alter the frequency and intensity of extreme meteorological events, in particular heat waves (Easterling et al. 2000), as well as droughts and floods (Tebaldi et al. 2006). These changes will interact with the non-linear seasonal dynamics of the host and parasite populations in ways that need to be better understood, in particular for vector-borne diseases and under intervention measures. New ‘emergent’ pathogens may also appear following increased opportunities for pathogens to jump from unrecognized reservoir host species to humans or domestic livestock; these ‘emergences’ are by definition ‘unpredictable’ but efforts are underway to identify environmental conditions that influence the likelihood of such events (Lloyd-Smith et al. 2009).
In this paper we compare the strengths and weaknesses of the current state-of-the-art forecasts systems for anticipating occurrence of infectious diseases and those for concomitant areas of climate research.
As many possible sources of climatic uncertainty are unimportant over a 20-year time scale (Stott and Kettleborough 2002; Friedlingstein et al. 2006), we will take advantage of the projections available to compare today’s climate with that in the 2030s. Twenty years is also an appropriate timescale for policy makers and stakeholders, as it balances scientific and political expediency. Everything we describe suggests that a more symbiotic interaction between climatologists and infectious disease ecologists needs to be urgently encouraged: the problems involved are scientifically challenging, but not unsolvable. The product of this synergistic interaction has the potential to mitigate and reduce significant levels of future human suffering.
1.1 Projected climate change for the next decades
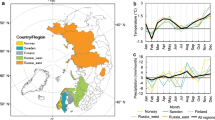
Figure 1 illustrates the uncertainty due to changes in temperature and precipitation for the decade ‘2021–30’ relative to the past decade (1997–2006) for different emission scenarios and each continent (see Fig. S1 and SI for the specific terminology used). Climate in the 2020s is projected to be warmer than today by about 0.49 °C, and by about 0.65 °C over land areas (see Fig. S1). Estimates of seasonal changes suggest that this warming will be noticeable and unusual even in such a near future. Major winter warming is projected to occur over North America, Asia and Europe and sustained temperature increases are projected for all regions. Estimated changes in precipitation are less clear than for temperature, as precipitation is inherently more variable (spatially and temporally) than temperature and because it does not respond so directly to greenhouse gas increases. Essentially the anthropogenic climate change over the next 20 years is largely predetermined, should a major tropical volcano not erupt, and projections for climate change through to the 2020s are fairly robust (Friedlingstein et al. 2006).

Changes in the seasonal cycle over continental regions for surface temperature (left) and precipitation (right) in the 2021–2030 decade with regard to the past decade (1997–2006). Colored line pairs denote the approximate 5th–95th percentile range across model simulations for the SRES A1B (gray, 33 simulations from 10 models), and SRES B1 (green, 22 from 8) emissions scenarios. See SI for more information
At local scales, climate change effects will reduce parasite generation time and potentially lead to increased peaks of transmission rate (e.g. through an increase in daily mean temperature (Harvell et al. 2002). Although it is also possible that large temperature peaks may overcome the pathogens metabolism at temperature peaks, this might create bi-modality in patterns of seasonal transmission. The window of transmission for seasonally driven parasitic species will increase in polar and temperate regions, as transmission seasons get warmer and longer and allow greater number of generations of parasites per year (Dobson et al. 2003; Kutz et al. 2005). Ultimately, this could also increase the rates of evolution of drug resistance, as shorter generation times allow the genetic structure of pathogen population to respond more rapidly to selection (May and Dobson 1986). In areas where cold seasons become both warmer and shorter with less frequent and less extreme cold spells we would expect this to enhance the ability of pathogens and their vectors to survive the winter, altering both their annual cycles of transmission intensity and their latitudinal and altitudinal distributions (Enserink 2007). Opposite to these effects there will also be some beneficial role for climate change as, for example, tick-borne encephalitis could be lost from large areas of central Europe if there were a change in the pattern of autumn cooling that would prevent nymph and larval ticks co-feeding at the same time (Randolph and Rogers 2000). Similarly, to some extent, increased awareness of infectious diseases and socio-economic development, may lead to increased investment by individuals and institutions on intervention measures to control disease risk (Lafferty 2009).
2 Current mechanistic approaches to climate and disease occurrence
The full quantification of the mechanisms accounting for the coupling of climate to the dynamics of infectious diseases is poorly served by the scarcity of long-term time-series. At present there are less than twenty long-term data sets for infectious diseases from which we can construct predictive models for regional disease outbreaks and that have been used repeatedly in a number of studies (see a detailed list in the SI). Shorter spatio-temporal records exist where the high spatial resolution can provide valuable information on disease dynamics (e.g., Chikungunya outbreaks of Reunión island, Boëlle et al. 2008; and the recent cholera epidemic in Haiti, Rinaldo et al. 2012).
Short-term (within a year) early-warning systems (EWS) for specific pathogens normally operate at a national or district level and require initial times series data for climate and disease incidence for initial parameterization. Increasingly, sea surface temperature (SST) anomalies in regions such as the tropical Indian and Pacific Oceans, on which indices for these climatic modes are based provide a source of predictability for the development of regional EWS of disease incidence at time scales of around 6 months, and occasionally a little longer (e.g. Cash et al. 2009a,b). On decadal time scales, more broad-scale predictions are slowly being generated that will eventually allow prediction of potential future distributions for a diversity of pathogens at a continental or global scale (Estrada-Peña and Venzal 2007). Uncertainty is inherent here as such projections also require knowledge of land use change and response of the pathogen to current and future control methods.
We can illustrate some of the challenges faced in interdisciplinary studies of climate-based projections for infectious diseases by examining where the uncertainties lie for both climate and epidemiological models. Initially consider how current skill of climate models differs at different spatial and temporal scales and geographic location (Fig. 2 and Figs. S2, S3, see caption of Fig. S2 and SI for a description of the methodology employed to evaluate this skill). At the very short time scales of hours to a few days, we can consistently say that the synoptic weather patterns are good predictors of what the weather will be in a few hours time at the same spatial location. However, as the time scale lengthens to weeks and a few months, the nonlinearities inherent in the climate system make detailed prediction much harder and skill declines (see for instance how mean skill changes in Fig. 2 for 2-metre temperatures, in different regions). Here it is important to note there are important differences between current skill in temperate and tropical systems: short-term climate prediction (weeks to a few months) is much better in the tropics than in mid-latitudes (see Fig. S2a, b in comparison to Figs. S2c–f and S3), mainly due to ENSO predictability. Similarly, seasonal-to-inter-annual skill is much better in the tropics than in the southern hemisphere (SH) temperate zone. In the SH, skill is similar to that in the NH, particularly beyond time scales of a few years. In addition, there is a decline in skill for surface temperature at the 3–6-yr timescale in the tropics (see SI), with skill over the longer time scales of a decade being similar for the tropics and the NH mid-latitudes, and lower in the SH (Fig. 2c). Results for individual seasons (DJF and JJA) for precipitation in the different latitude regions offer similar conclusions as those above (high skill in the tropics, lower skill in temperate regions in the first couple of years, large role of the long-term trends as time scales approach 10 years) (Fig. S3). Current decadal climate prediction systems (Doblas-Reyes et al. 2010, 2011) provide reasonable hope that obtaining sufficiently accurate forecasts of inter-annual-to-decadal changes in climate-sensitive diseases is already possible. Beyond the time scale offered by the decadal predictions, projections for the next decades suggest that climate change will be more dramatic and well defined at the poles, but significantly less well defined, with higher variability in the tropics and temperate zones. Near-term predictions may have very little skill at small spatial scale. Although transmission models for seasonal and interannual prediction could lengthen their lead times by incorporating climate predictions rather than observations, this would ideally require detailed forecasts for at least temperature and rainfall at a resolution of about one to ten square kilometers, which is not currently available. In addition, the value of seasonal forecasts is constrained by the predictive skill of epidemiological models. Let us consider a hypothetical vector-transmitted pathogen, such as for malaria, dengue, or West Nile. These are pathogens whose development times in their vectors are highly sensitive to temperature, while vector abundance is in turn dependent upon births, which are often highly sensitive to rainfall, while vector survival may non-linearly be dependent upon temperature. We can usually define with reasonable skill regions where these pathogens cannot persist, essentially this is defined by the boundary where temperature is too cold for pathogen development during the course of host life expectancy. Models considering this type of constraint were used to produce early predictive maps for expansion of vector borne disease in the face of climate change (Gillett 1974; Martens et al. 1997). Similarly, models exhibit reasonable skill in predicting the prevalence of pathogens in areas where they are hyperendemic and climate conditions produce relatively simple annual cycles of prevalence and incidence. Predictions become complicated but still feasible at the boundary regions where transmission is low and the pathogen establishes only transiently during times of the year when climate conditions allow vector abundance to reach levels where transmission of rapidly developing pathogens is effective (e.g. Baeza et al. 2011). Here, probabilistic projections of epidemic risk can in some cases be made effectively on the basis of climate variables, such as rainfall or associated vegetation indices from remote sensing (e.g. Thomson et al. 2006; Laneri et al. 2010). Predictions of disease incidence become more challenging in between these two extremes, in regions that are hypo- to meso-endemic where the pathogen can exhibit more nonlinear dynamics. The build-up and decline of herd-immunity in the host population (proportion of hosts that are immunologically resistant) is a key non-linear determinant of potential to predict future outbreaks and their size (e.g. Bjornstad and Grenfell 2001; Koelle and Pascual 2004).

Ensemble-mean correlation skill of 2-metre air temperature predictions obtained with the DePreSys forecast system and NCEP/NCAR reanalysis. Forecast-time average is expressed in months, up to 10 years. Y-axis in all panels reflects spatial scale of aggregation, thus larger values indicate larger spatial scales. a Tropics (20S-20N), b NH (20N-60N), c SH (20S-60S)
One way to quantify the influence of climate variability on rates of transmission relates to the reproductive number of an infectious disease (known asR0) and consists of examining changes in infection with host age and then predicting how climate-driven changes in transmission affect this relationship (Hudson and Dobson 1995; see SI). Related quantities that consider only part of the transmission cycle by focusing on the vector, such as vectorial capacity (the mean number of potentially infective contacts made by a mosquito population per infectious person per unit time) and the critical density threshold of vector populations, have also been used to produce risk maps as a function of climate change (e.g. for dengue fever, Jetten and Focks 1997). Initial efforts that used this approach projected alarming increases in geographical range (Martens et al. 1997) and were criticized for lack of a proper validation and for violating assumptions about how R0 should be measured under conditions where the pathogen is firmly established (e.g. Rogers and Randolph 2000). A number of more recent efforts have taken important steps towards validation by estimating the current distributions and burdens of disease incidence; they remain limited by the paucity of data available at appropriate scales for cross-validation (Peterson and Shaw 2003; Tanser et al. 2003; Jetten and Focks 1997; Snow et al. 1999). Mechanistic models for the population dynamics of infectious diseases provide the basis for the development of increasingly sophisticated suitability indices to delineate the geographic distribution of suitable habitat given by environmental constraints, such as temperature and precipitation for malaria, and how this distribution would vary in time as the result of climate change (Gething et al. 2011). This use of transmission models should continue, together with efforts to validate the distributions produced by resulting indices in both time and space, including the characterization of the temporal scales at which they are able to capture relevant variation (Pascual and Bouma 2009).
3 Resolving the interplay between transmission, host immunity and intervention measures
The population dynamics of cholera, malaria and other key water-borne, and vector-transmitted pathogens have the potential to resonate with both annual and longer-term climate cycles to produce more complex patterns of long-term epidemic behaviour (Pascual et al. 2000; Rogers and Randolph 2000). It has been recognized that herd-immunity, and the associated propensity of disease dynamics to oscillate with the waxing and waning of herd immunity in the host population, can place significant constraints on the ability of simple, correlative analyses to detect potential climate signals in time series records for important tropical diseases (Rogers et al. 2002; Pascual et al. 2008; Childs and Boots 2010). Quantitative approaches beyond traditional linear correlative ones have been developed to retrospectively disentangle the effects of endogenous disease dynamics, for example, as the result of ‘herd’ immunity, vs. exogenous drivers such as climate variability (Pascual et al. 2000; Rodó et al. 2002; Koelle et al. 2005; Stenseth et al. 2006).
Our understanding of how herd immunity interacts with seasonal (and interannual) forcing of transmission has been strongly shaped by the extensive studies of the nonlinear (SIR) dynamics of childhood diseases, such as measles and whooping cough (Earn et al. 2000; Bjornstad and Grenfell 2001). Lessons learnt may not transfer in a simple way to the case of vector-borne infections, because of the more complex transmission cycle as well as the more complex nature of immunity acquisition and loss that is intimately related to the antigenic diversity of the parasite (Fig. S4). Figure S4 illustrates that the decoupling between incidence and climate forcing in a model of malaria transmission that incorporates parasite diversity in the form of superinfection (Dietz et al. 1974). Although this decoupling occurs as expected in an intermediate window of transmission intensities, and more importantly, it can be weak and occur in a narrow window of parameter space. Moreover, the potential for this decoupling depends critically on both vector parameters and properties of the environment (such as topography and hydrology influencing vector recruitment as a function of rainfall). Superinfection, which enhances the maintenance of immunity, and chronic infection through repeated exposure, also influences the nonlinearities in the relationship between climate variability and transmission dynamics. This is a key area that should be addressed in the future with epidemiological models specifically tailored to vector-transmitted diseases that produce short-term immunity to multiple strains of the pathogen, which may illicit complementary immunological protection. One conjecture is that for efficient vectors and environments, the intermediate range of climatic parameters in which a decoupling might occur is in practice small, and bracketed by regimes for which infection levels are either too low for ‘herd’ immunity to dynamically matter, or those in which superinfection and the availability of partially immune hosts dampen intrinsic oscillations. Nevertheless, these intermediate regions are of particular relevance to the impact of both intervention measures and climate variability, as they represent transition regions that must be crossed from high endemicity towards eradication, and from fringe areas such as highlands where temperature previously limited transmission towards more favourable climate conditions. They may also be areas where people have initially selectively settled to develop agriculture while escaping the continued impact of infectious diseases.
Moreover, model structure can now be more closely tailored to specific diseases, and include in particular the explicit representation of human intervention to interrogate retrospective data on multiple drivers as well as on their interaction. The interaction of control efforts with climate variability should be of particular relevance when intervention measures are implemented in response to previous increases in incidence, for example for residual insecticide spraying in desert malaria in NW India (Baeza et al. 2011). Such reactive control is potentially another source of nonlinearity that creates cycles in epidemiological dynamics. Furthermore any form of partially effective control can substantially weaken the climate signal in disease data, while simultaneously masking increases in transmission driven by climate variability. The nonlinearities induced by human behaviour and limited resources for intervention, are likely to play a more important role than those generated by herd immunity in highly seasonal environments with low transmission. Intervention measures will also be closely linked to socio-economic conditions and introduce important long-term trends whose role in modifying projections for disease risk based on climate change will be an important area of study. These conditions are central to the multivariate character of change in infectious diseases illustrated for example by the case study of tick-borne encephalitis in Europe (Randolph and Rogers 2000). In this context, transmission models complement statistical analyses in providing useful tools to isolate the putative effects of climate variables and to examine how other factors would modify these effects.
Host immunity also plays a much smaller role in the dynamics of pathogens that utilize small mammals and birds as reservoir hosts (such as Hanta virus, Plague, leptospirosis and West Nile virus, e.g. Bell et al. 2005, 2006). Here the birth and death rates of the host populations operate at a sufficiently rapid level that immune hosts die and are replaced by young naïve hosts at too high a rate for any significant level of herd immunity to build up (although herd-immunity may be important at transient seasonal time scales for pathogens such as West Nile virus; see Fig. S5 and Hosseini 2006). Thus the dynamics of systems with short-lived mammalian and avian reservoirs are probably much more strongly influenced by climate driven host recruitment; in these systems climate conditions that promote fecundity can cause systems to cross the thresholds that promote infectious disease outbreaks. Seasonality in host demography and social behaviour, as well as climate driven variations in vector and infective stage viability create a number of nonlinear thresholds that modulate disease transmission (Kausrud et al. 2007). Examples of such thresholds are found in the increase of leptospirosis and chikungunya with rainfall (Altizer et al. 2006; Boëlle et al. 2008) and in the relationship between the different vital parameters of vectors and temperature, such as the lower temperature limit for the development of malaria in mosquitoes (Gilles 1999).
4 Can climate research help in future prediction of disease occurrence?
The latest multi-national assessment of the risks associated with climate change (IPCC 2007), adopted a probabilistic framework that more directly addresses the issue of prediction uncertainty (Friedlingstein et al. 2006); this is key for the delivery of useful disease incidence projections. There is considerable geographic variation in our ability to make probabilistic predictions from multi-model ensemble (MME) systems for temperature (A) and precipitation (B) subtropical areas and for selected regions in the mid-latitudes (Fig. 3, but see also Fig. S6). These largely correspond to regions where vector-and water borne-diseases are endemic and also to areas where we have seen recurrent outbreaks of climate driven diseases reported to the WHO in recent years (Palmer et al. 2009; World Health Organization WHO 2004, 2006). Although there are significant areas with important pathogens where the climate models exhibit low, or null, prediction skill, it is true also that in many key areas there is high potential to make climate forecasts at temporal and spatial scales that could be used in predictive epidemiological models. The MME system is particularly relevant as it shows high skill in its ability to predict El Niño events several months in advance (Fig. 3c). Therefore, the development and implementation of regional to local early-warning systems may soon be within reach for pathogens such as cholera that are significantly driven by the impact of ENSO in local weather (Koelle et al. 2005).

The Relative Operating Characteristic (ROC) Skill (positive ROC skill score statistically significant with 95 % confidence) for 1-month lead seasonal probabilistic predictions of anomalies of a precipitation and b temperature above the upper tercile in winter. Superimposed to the skill maps for the different variables are the current distribution of the main CD infectious diseases (namely malaria, dengue and cholera) and the location of epidemic outbreaks of CD diseases between 2004 and 2006 according to the WHO. c MME prediction for the last 20 years of el Nino3.4 anomalies, validated against ERA40. Note the good skill in anticipating ENSO, one of the predominant drivers of CD diseases currently incorporated in predictive models. Green bars denote terciles in spread of predictions
While at decadal time scales, a majority of models seem to consistently estimate a future warming in the Niño 3.4 ENSO region (see Fig. S1c), their projections instead for the degree of associated changes in interannual variability over land can differ considerably both within, and between, different region (WHO 2006).
A variety of vectors and pathogens might be sensitive to extremes of climate and to gradual changes in weather patterns. As a consequence, improving disease modelling can require climate information far more detailed than regional seasonal mean temperature and precipitation. Sustained heat waves and long-lasting weather events, although not necessarily unusual in magnitude (Stige et al. 2007), can increase the risk of outbreaks of vector-borne and other infectious diseases due to changes in patterns of human behaviour, physical stress, or the breakdown of sanitary services (D’Souza et al. 2004; Ballester et al. 2003).
There is evidence from both observations and climate simulations that extreme daily precipitation frequency is growing in the extra-tropics (see Fig. S6), even in regions that are experiencing a dryer climate. The impact of this is increasingly evident around the globe with exceptional floods and droughts currently occurring in many areas: India, Europe, California and Australia (Tebaldi et al. 2006; Zell 2004). The impacts of such changes on human health in the future decades will largely depend on the disease considered, its epidemic or endemic nature, the varying susceptibility of the human population especially in the large cities of the developing world (Reiner et al. 2012), and the response of public health systems when trying to buffer its effects. Similarly, droughts pose another interesting challenge to our prediction capacity, as diseases associated with this sort of rainfall extreme, demand a proper integration of satellite imaging and remote sensing information into models and early-warning systems. A clear example is meningococcal meningitis in sub-Saharan Africa (Greenwood et al. 1984),
Regional heat waves are also seen to be increasing in intensity and duration (Chew et al. 1998; Meehl and Tebaldi 2004) as well as in spatial extent (Stott 2004), with known projected effects on human mortality (Ballester et al. 2011). As future changes in heat waves appear intimately linked to global warming, these trends are expected to intensify in the following decades for all land regions (IPCC, IPCC 2007) (see Fig. S7c). What is especially interesting for pathogen transmission is that night-time temperatures drive much of this extreme heating and might be particularly important for reducing pathogen and vector generation times. This is consistent with larger observed increases in minimum temperatures observed in some regions (Ballester et al. 2003), compared to maximum temperatures (Easterling et al. 2000; Gershunov and Douville 2013). Despite their potential importance, there have been no direct studies of the effect of extremes on the dynamics of infectious diseases, though the effect has been sometimes suggested (e.g. for extreme rainfall and outbreaks of Escherichia coli 0157:H7, Cryptosporidium (Lobell et al. 2007; Charron et al. 2004; Rose et al. 2002; Curriero et al. 2001), tiphoid hepatitis, salmonellosis and leptospirosis. Conversely, both observations and models suggest that the frequency of frost days is decreasing everywhere (Tebaldi et al. 2006); this provides increased opportunities for tropical diseases and plant pests to penetrate into the mid-latitudes. These more frequent and spatially extensive crossing of climatic thresholds, can also potentially trigger nonlinear increases in rates of pathogen transmission and evolution. Furthermore, the increasing spatial scale of heat waves or floods can synchronize infectious disease outbreaks over broader areas (Curriero et al. 2001; Cazelles et al. 2005) posing increasing pressure over the public health system. One such example were catastrophic floods in several countries of Africa, with all of them showing large cholera epidemics in phase with rainfall extremes (de Magny et al. 2007).
Combination of climate effects and human actions (be they directly effected on the environment, or as a result of changes in social behaviour, such as migration, displacement or social conflicts), may lead to unprecedented and unpredictable expansions of disease ranges. In fact, some diseases for which parasites or vectors are already eliminated in an area and for which there is no build-up immunity left within the population, may reappear as a consequence of combined global and climate change effects.
5 Top future research priorities
In order to improve future studies linking climate change and infectious diseases, we suggest the following research priorities:
-
1-
Establish a suite of long-term, surveillance sites where key indices of pathogen transmission and human health are routinely collected on a weekly (preferably), or monthly, basis (disease incidence, vector populations and complete demographic characterization of local human populations: births, deaths and immigration). This sampling should be done in conjunction with all possible ground-based meteorological monitoring and the simultaneous gathering of long-term retrospective climate data.
-
2-
Sites in 1) should be located in both epidemic and endemic areas, preferably forming a transect covering the disease gradient. For epidemic situations, the fringes of transmission areas, such as arid and highland regions for malaria, are especially sensitive to climate forcing. Key indicators of other components of global change should also be monitored: land-use change, water availability, demography and socio-economic status. In endemic sites, changes in disease dynamics should be tracked paying particular attention to changes in the structure, in particular the age distribution of outbreaks.
-
3-
Undertake comparative analyses that enable cross-testing of the sensitivity and skill of different types of climate-driven disease models. In particular, develop stronger intercomparison experiments among statistical, semi-mechanistic, and fully dynamic models to derive credible probabilistic projections of disease incidence.
-
4-
Develop better ways to estimate confidence limits and natural bounds for fluctuations in parameters that are critical for constraining base conditions for disease models. This information should come from field surveys and experiments in central disease areas. In particular probabilistic (Bayesian) projections need to be developed that restrict the range of parameter estimates on the basis of available information.
-
5-
Investigate in a series of case studies for different infectious diseases the key question of the spatial and temporal resolution at which associations with climate variability are most evident and early-warning systems exhibit best skill. Some examples of diseases and locations for which such analyses might be undertaken are cited above and in the SI However, the critical property of the data sets would be a combination of sufficient spatial resolution with spatial and temporal extent.
-
6-
Investigate strategies to generate skilful seasonal-to-decadal disease predictions. Such strategies should address the mismatch between the spatial resolutions required by epidemiological modellers and those that are currently possible in climate products, especially given the importance of a good representation of variability and skill at seasonal and inter-annual time scales.
-
7-
Develop a new class of semi-mechanistic models with limited parameters to minimize confounding effects of over-parameterization. Current approaches tend either to include a myriad of parameters that cannot realistically be specified in ordinary differential equations (ODE) systems, or conversely, use over-simplistic statistical methodologies that are simply extrapolated, and provide little expectation of success in the future for different environmental ranges.
-
8-
Develop a set of new scenarios for the future of selected infectious diseases driven by climate that incorporate different levels of mitigation and adaptation strategies.
Human health and climate change are usually treated as separate agendas by government policy makers and funding agencies. Unfortunately it is likely that the two are intimately linked and climate change will increasingly exacerbate infectious disease problems. Considerable progress has been made in the development of models for pathogens such as cholera and malaria where climate plays key roles in driving transmission. The full-scale implementation of symbiotic climate driven disease projections is unfortunately currently limited by the paucity of long-term data sets available to accurately structure and parameterize the next generation of predictive epidemic models. Collating and starting to collect better resolved epidemiological data for climate sensitive diseases will allow us to develop more efficient ways of more efficiently focusing and utilizing the limited means of intervention available for tropical diseases. Ultimately this should be of the highest priority in the future battle against the diseases that continue to place the greatest burden on the world’s poorest people and the economies of the countries in which they live (May 2007).
References
Alonso D, Bouma M, Pascual M (2011) Epidemic malaria and warmer temperatures in recent decades in an East African highland. Proceedings of the Royal Society B. doi:10.1098/repb.2010.2020
Altizer S, Dobson A, Hosseini P, Hudson P, Pascual M, Rohani P (2006) Seasonality and population dynamics: Infectious diseases as case studies. Ecology Letters 9:467–484
Baeza A, Bouma MJ, Dobson AP, Dhiman R, Srivastava HC, Pascual M (2011) Climate forcing and desert malaria: the effect of irrigation. Mal J 10:190
Ballester F, Michelozzi P, Iniguez C (2003) Weather, climate, and public health. Journal of Epidemiology and Community Health 57:759–760
Ballester J, Robine J-M, Hermann F, Rodó X (2011) Long-term projections and acclimatization scenarios of temperature-related mortality in Europe. Nat Comms 2:358. doi:10.1038/ncomms1360
Bell JA, Mickelson NJ, Vaughan JA (2005) West Nile virus in hostseeking mosquitoes within a residential neighborhood in Grand Forks, North Dakota. Vector Borne Zoonotic Dis 5:373–382. doi:10.1089/vbz.2005.5.373
Bell JA, Brewer CM, Mickelson NJ, Garman GW, Vaughan JA (2006) West Nile virus epizootiology, central Red River Valley, North Dakota and Minnesota, 2002–2005. Emerg. Infect. Dis. Available from http://www.cdc.gov/ncidod/EID/vol12no08/06-0129.htm
Bjornstad ON, Grenfell BT (2001) Noisy clockwork: Time series analysis of population fluctuations in animals. Science 293(5530):638–643
Boëlle PY, Thomas G, Vergu E, Renault P, Valleron AJ, Flahault A (2008) Investigating transmission in a two-wave epidemic of Chikungunya fever, Reunion Island. Vector Borne Zoonotic Dis 8:207–218
Cash BA, Rodó X, Kinter JL III (2009a) Links between tropical Pacific SST and the regional climate of Bangladesh: Role of the western tropical and central extratropical Pacific. J Clim 22:1641–1660
Cash BA, Rodo X, Kinter JL III (2009b) Links between tropical pacific SST and Cholera Incidence in Bangladesh: Role of the western tropical and central extratropical pacific. J Clim 22(7):1641–1660
Cazelles B, Chavez M, McMichael AJ, Hales S (2005) Nonstationary Influence of El Niño on the Synchronous Dengue Epidemics in Thailand. PLoS Med 2(4):313–318
Charron DF, Thomas MK, Waltner-Toews D, Aramini JJ, Edge T, Kent RA, Maarouf AR, Wilson J (2004) Vulnerability of waterborne diseases to climate change in Canada: A review. Journal of Toxicology and Environmental Health—Part A: Current Issues 67(20–22):1667–1677
Chew FT, Doraisingham S, Ling AE, Kumarasinghe G, Lee BW (1998) Seasonal trends of viral respiratory tract infections in the Tropics. Epidemiol Infect 121:121–128
Childs DZ, Boots M (2010) Seasonal forcing, immunity and the dynamics of malaria. Royal Society Interface 7:309–319
Curriero FC, Patz JA, Rose JB, Lele S (2001) The association between extreme precipitation and waterborne disease outbreaks in the United States, 1948–1994. American Journal of Public Health 91(8):1194–1199
D’Souza RM, Beeker NG, Hall G, Moodie KBA (2004) Does ambient temperature affect foodborne disease? Epidemiology 15(1):86–92
de Magny GC, Guégan J-F, Petit M, Cazelles B (2007) Regional-scale climate variability synchrony of cholera epidemics in West Africa BMC Infectious Diseases 7:20
Dietz K, Molineax L, Thomas A (1974) Malaria model tested in African savannah (1974). Bulletin of the World Health Organization
Doblas-Reyes FJ, Weisheimer A, Palmer TN, Murphy JM, Smith D (2010) Forecast quality assessment of the ENSEMBLES seasonal-to-decadal Stream 2 hindcasts. ECMWF Tech Memo 621:45, Reading UK
Doblas-Reyes FJ, Balmaseda MA, Weisheimer A, Palmer TN (2011) Decadal climate prediction with the ECMWF coupled forecast system: Impact of ocean observations. Journal Geophysical Research A 116:D19111. doi:10.1029/2010JD015394
Dobson AP, Kutz S, Pascual M, Winfree R (2003) Pathogens and parasites in a changing world. In: Lovejoy T (ed) Climate change and biodiversity: Synergistic impacts. Yale University Press, New Haven
Earn DJ, Rohani P, Bolker BM, Grenfell BT (2000) A simple model for complex dynamical transitions in epidemics. Science 287(5453):667–670
Easterling DR, Evans JL, Groisman P, Karl TR, Kunkel KE, Ambenje P (2000) Observed variability and trends in extreme climatic events: a brief review. Bulletin of the American Meteorological Society 81:417–425
Enserink M (2007) Tropical disease follows mosquitoes to Europe. Science 317:1485
Estrada-Peña A, Venzal JM (2007) Climate niches of tick species in the Mediterranean region: modeling of occurrence data, distributional constraints, and impact of climate change. J Med Entomol 44:1130–1138
Friedlingstein P, Cox P, Betts R, Bopp L, von Bloh W, Brovkin V, Cadule P, Doney S, Eby M, Fung I, Bala G, John J, Jones C, Joos F, Kato T, Kawamiya M, Knorr W, Lindsay K, Matthews HD, Raddatz T, Rayner P, Reick C, Roeckner E, Schnitzler K-G, Schnur R, Strassmann K, Weaver AJ, Yoshikawa C, Zeng N (2006) Climate-carbon cycle feedback analysis: Results from the C4MIP model intercomparison. J Climate 19:3337–3353
Gershunov A, Douville H (2013) Extensive summer hot and cold extremes under current and possible future climatic conditions: Europe and North America. In: H. Diaz and R. Murnane (Eds), Climate Extremes and Society. Cambridge University Press
Gething PW, Van Boeckel TP, Smith DL, Guerra CA, Patil AP, Snow RW, Hay SI (2011) Modelling the global constraints of temperature on transmission of Plasmodium falciparum and P. vivax Parasites & Vectors 4:92 doi:10.1186/1756-3305-4-92
Gilles (1999) Epidemiology. Oxford University Press, Oxford
Gillett JD (1974) Direct and indirect influences of temperature on the transmission of parasites from insects to man. The Effects of Meteorological Factors upon Parasites. A. E. R. Taylor and R. Muller. Blackwell Scientific, Oxford, Symposia of the British Parasitological Society 12:79–95
Greenwood BM, Blakebrough IS, Bradley AK, Wali S, Whittle HC et al (1984) Meningococcal disease and season in sub-Saharan Africa. Lancet 1:1339–1342
Harvell CD, Mitchell CE, Ward JR, Altizer S, Dobson AP, Ostfeld RS, Samuel MD (2002) Climate Warming and Disease Risks for Terrestrial and Marine Biota Science 296:2158–2162
Hosseini PR (2006) Pattern formation and individual-based models: the importance of understanding individual-based movement. Ecol Mod 194:357–371
Hudson PJ, Dobson AP (1995) Macroparasites: Observed patterns in naturally fluctuating animal populations. In: Grenfell BT, Dobson AP (eds) Infectious diseases in natural populations. Cambridge University Press, Cambridge, pp 144–176
IPCC (2007) The physical science basis. In: Solomon S et al (eds) Contribution of working Group I to the fourth assessment report of the intergovernmental panel on climate change. Cambridge University Press, Cambridge
Jetten TH, Focks DA (1997) Potential changes in the distribution of dengue transmission under climate warming. American Journal of Tropical Medicine and Hygiene 57:285–297
Kausrud KL, Viljugrein H, Frigessi A, Begon M, Davis S, Leirs H, Dubyanskiy V, Stenseth NC (2007) Climatically-driven synchrony of gerbil populations allows large-scale plague outbreaks. Proceedings of the Royal Society of London, B 274:1963–1969
Koelle K, Pascual M (2004) Disentangling extrinsic from intrinsic factors in disease dynamics: A nonlinear time series approach with an application to cholera. The American Naturalist 163(6):901–913
Koelle K, Rodó X, Pascual M, Yunus MD, Mostafa G (2005) Refractory periods and environmental forcing in cholera dynamics. Nature 436:696–700
Kutz SJ, Hoberg EP, Polley L, Jenkins EJ (2005) Global warming is changing the dynamics of Arctic host-parasite systems. Proceedings of the Royal Society of London B, Published Online, doi:10.1098
Lafferty KD (2009) The ecology of climate change and infectious diseases: Ecology, v. 90, no. 4, p. 888–900, doi:10.1890/08-0079.1
Laneri K, Bhadra A, Ionides EL, Bouma M, Dhiman RC et al (2010) Forcing Versus Feedback: Epidemic Malaria and Monsoon Rains in Northwest India. PLoS Comput Biol 6(9):e1000898. doi:10.1371/journal.pcbi.1000898
Lloyd-Smith JO, George D et al (2009) Epidemic dynamics at the human-animal interface. Science 326(5958):1362–1367
Lobell DB, Cahill KN, Field CB (2007) Historical effects of temperature and precipitation on California crop yields. Climatic Change 81:187–203
Martens WJM, Jetten TH, Focks DA (1997) Sensitivity of malaria, schistosomiasis and dengue to global warming. Climate Change 35:145–156
May RM (2007) Parasites, people and policy: Infectious diseases and the millennium development goals. Trends in Ecology and Evolution 22(10):497–503
May RM, Dobson AP (1986) Population dynamics and the rate of evolution of pesticide resistance. pp. 170–193 in Pesticide Resistance Management. NAS-NRC Publications (from an International Symposium, Washington, D.C., 27–29 November 1984).
Meehl GA, Tebaldi C (2004) More intense, more frequent, and longer lasting heat waves in the twenty-first century. Science 305:994–997
Palmer TN, Doblas-Reyes FJ, Weisheimer A, Rodwell M (2009) Towards “seamless” prediction: Calibration of climate-change projections using seasonal forecasts. Bulletin of the American Meteorological Society 89:459–470
Pascual M, MJ Bouma (2009) Do rising temperatures matter? Ecology 90(4):906–912
Pascual M, Rodo X, Ellner SP, Colwell R, Bouma MJ (2000) Cholera dynamics and the El Niño Southern Oscillation. Science 289(5485):1766
Pascual M, Chaves LF, Cash B, Rodó X, Yunus MD (2008) Predicting endemic cholera: The role of climate variability and disease dynamics. Clim Res 36:131–140
Peterson AT, Shaw J (2003) Lutzomyia vectors for cutaneous leishmaniasis in Southern Brazil: Ecological niche models, predicted geographic distributions, and climate change effects. International Journal for Parasitology 33:919–931
Randolph SE, Rogers DJ (2000) Fragile transmission cycles of tick-borne encephalitis virus may be disrupted by predicted climate change. Proc R Soc Lond B Biol Sci 267:1741–1744
Reiner R, King A, Emch M, Yunus M, Faruque A, Pascual M (2012) Highly localized sensitivity to climate forcing drives endemic cholera in a megacity. PNAS Early Edition. doi:10.1073/pnas.1108438109
Rinaldo A, Bertuzzo E, Mari L, Righetto L et al (2012) Reassessment of the 2010–2011 Haiti cholera outbreak and rainfall-driven multiseason projections. PNAS. doi:10.1073
Rodó X, Pascual M, Fuchs G, Faruque ASG (2002) ENSO and cholera: A nonstationary link related to climate change? PNAS 99:12901–12906
Rogers DJ, Randolph SE (2000) The Global Spread of Malaria in a Future. Warmer World Science 289:1763–1766
Rogers D, Randolph SE, Snow RW, Hay SI (2002) Satellite imagery in the study and forecast of malaria. Nature 415:710–715
Rose JB, Huffman DE, Gennaccaro A (2002) Risk and control of waterborne cryptosporidiosis. FEMS Microbiology Reviews 26(2):113–123
Snow RW, Craig MH, Deichmann U, le Sueur D (1999) A Preliminary Continental Risk Map for Malaria Mortality among African Children. Parasitology Today 15(3):99–104
Stenseth NC, Samia NI, Viljugrein H, Kausrud K, Begon M, Davis S, Leirs H, Dubyanskiy VM, Esper J, Ageyev VS, Klassovskiy NL, Pole SB, Chan KS (2006) Plague Dynamics are driven by climate variation. Proceedings of National Academy of Sciences 103:13110–13115
Stige LC, Chan K-S, Zhang Z, Frank D, Stenseth NC (2007) Thousand-year-long Chinese time series reveals climatic forcing of decadal locust dynamics. Proceedings of the National Academy of Sciences 104:16188–16193
Stott P (2004) A, Stone, D.A. & Allen, M.R. Human contribution to the European heat wave of 2003. Nature 432:610–613
Stott PA, Kettleborough JA (2002) Origins and estimates of uncertainty in predictions of twenty-first century temperature rise. Nature 416:723–726
Tanser FC, Sharp B, le Sueur D (2003) Potential effect of climate change on malaria transmission in Africa. Lancet 362:1792–1798
Tebaldi C, Hayhoe K, Arblaster JM, Meehl GA (2006) Going to the extremes: An intercomparison of model-simulated historical and future changes in extreme events. Clim Change 79:185–211
Thomson MC, Doblas-Reyes FJ, Mason SJ, Hagedorn R, Connor SJ, Phindela T, Morse A, Palmer TN (2006) Malaria early warnings based on seasonal climate forecasts from multi-model ensembles. Nature 439:576–579
World Health Organization (WHO). Global Health Atlas, http://www.who.int/globalatlas/ (2004).
World Health Organization (WHO). Global Health Atlas, http://www.who.int/globalatlas/ (2006).
Zell R (2004) Global climate change and the emergence/re-emergence of infectious diseases. International Journal of Medical Microbiology 293:16–26
Acknowledgements
The authors want to thank the La Caixa Foundation and in particular, Paquita Ciller, for the support received to host and fund the meeting on climate, populations and infectious diseases held at the COSMOCAIXA museum in Barcelona, in November, 2006. We also thank Kyrre l. Kausrud, Sunetra Gupta, Kevin Lafferty, Menno Bouma, D. Volpi and three Anonymous Referees for many useful discussions and comments on earlier versions of the manuscript. FJDR received financial support from the ENSEMBLES project (GOCE-CT-2003-505539). Support for this work was also provided by CIRCE-EUFP6 to X.R., by NIH/NSF EID Grant 0430120 and a NOAA award to X.R., M.P., J.K. and A.J.D. J.G-S and X. Rodó wants to acknowledge support from the EU project QWeCI (Quantifying Weather and Climate Impacts on health in developing countries; funded by the European Commission’s Seventh Framework Research Programme under the grant agreement 243964). and the DENFREE: DENgue research Framework for Resisting Epidemics in Europe of the EUFP7 programme project. M. Pascual is an investigator of the Howard Hughes Medical Institute.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Materials
Below is the link to the electronic supplementary material.
ESM 1
(PDF 2440 kb)
Rights and permissions
About this article
Cite this article
Rodó, X., Pascual, M., Doblas-Reyes, F.J. et al. Climate change and infectious diseases: Can we meet the needs for better prediction?. Climatic Change 118, 625–640 (2013). https://doi.org/10.1007/s10584-013-0744-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10584-013-0744-1