
Abstract
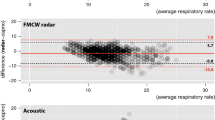
Respiratory rate has been shown to be an important predictor of cardiac arrest, respiratory adverse events and intensive care unit admission and has been designated a vital sign. However it is often inadequately monitored in hospitals. We test the hypothesis that RespiraSense, a piezoelectric-based novel respiratory rate (RR) monitor which measures the differential motion of the chest and abdomen during respiratory effort, is not inferior to commonly used methods of respiratory rate measurement. Respiratory rate was compared between the developed RespiraSense device and both electrocardiogram and direct observation by nursing staff. Data was collected from 48 patients admitted to the post-anaesthesia care unit in a tertiary level hospital. The primary outcome measure was difference in average RR calculated over a 15 min interval between (1) RespiraSense and ECG and (2) RespiraSense and nurses’ evaluation. The secondary outcome measure was the correlation between the respiratory rates measured using these three methods. The 95 % confidence interval for the difference in average RR between RespiraSense and ECG was calculated to be [−3.9, 3.1]. The 95 % confidence interval for the difference in average RR between RespiraSense and nurses’ evaluation was [−5.5, 4.3]. We demonstrate a clinically relevant agreement between RR monitored by the RespiraSense device with both ECG-derived and manually observed RR in 48 post-surgical patients in a PACU environment.






Similar content being viewed by others
References
Hillman K, Chen J, Cretikos M, et al. MERIT study investigators. Introduction of the medical emergency team (MET) system: a cluster randomised controlled trial. Lancet. 2005;365:2091–7.
National confidential enquiry into patient outcome and death. An acute problem? London: NCEPOD. http://www.ncepod.org.uk/2005.htm (2005). Accessed 22 June 2014.
Hodgetts TJ, Kenward G, Vlachonikalis IG, et al. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team. Resuscitation. 2002;54:125–31.
McBride J, Knight D, Piper J, et al. Long-term effect of introducing an early warning score on respiratory rate charting on general wards. Resuscitation. 2005;65:41–4.
Ryan H, Cadman C, Hann L. Setting standards for assessment of ward patients at risk of deterioration. Br J Nurs. 2004;13:1186–90.
Hogan J. Why don’t nurses monitor the respiratory rates of patients? Br J Nurs. 2006;15:489–92.
Fieselmann JF, Hendryx MS, Helms CM, et al. Respiratory rate predicts cardiopulmonary arrest for internal medicine patients. J Gen Intern Med. 1993;8:354–60.
Goldhill DR, McNarry AF, Mandersloot G, et al. A physiologically-based early warning score for ward patients: the association between score and outcome. Anaesthesia. 2005;60:547–53.
Subbe CP, Davies RG, Williams E, et al. Effect of introducing the Modified Early Warning score on clinical outcomes, cardio-pulmonary arrests and intensive care utilisation in acute medical admissions. Anaesthesia. 2003;58:797–802.
Cretikos M, Chen J, Hillman K, et al. The objective medical emergency team activation criteria: a case–control study. Resuscitation. 2007;73:62–72.
Overdyk FJ, Carter R, Maddox RR, et al. Continuous oximetry/capnometry monitoring reveals frequent desaturation and bradypnea during patient-controlled analgesia. Anesth Analg. 2007;105:412–8.
Taenzer AH, Pyke JB, McGrath SP, et al. Impact of pulse oximetry surveillance on rescue events and intensive care unit transfers: a before-and-after concurrence study. Anesthesiology. 2010;112:282–7.
Whitaker DK. Time for capnography–everywhere. Anaesthesia. 2011;66(7):544–9.
Kodali BS. Capnography outside the operating rooms. Anesthesiology. 2013;118(1):192–201.
Edmonds ZV, Mower WR, Lovato LM, et al. The reliability of vital sign measurements. Ann Emerg Med. 2002;39:233–7.
Folke M, Cernerud L, Ekström M, et al. Critical review of non-invasive respiratory monitoring in medical care. Med Biol Eng Comput. 2003;41:377–83.
Lovett PB, Buchwald JM, Stürman K, et al. The vexatious vital: neither clinical measurements by nurses nor an electronic monitor provides accurate assessments of respiratory rate in triage. Ann Emerg Med. 2005;45:68–76.
Ouchterlony J, Arvidsson S, Sjöstedt L, et al. Peroperative and immediate postoperative adverse events in patients undergoing elective general and orthopaedic surgery: the Gothenburg study of perioperative risk (PROPER). Part II. Acta Anaesthesiol Scand. 1995;39:643–52.
Rose D, Cohen M, Wigglesworth D, et al. Critical respiratory events in the postanesthesia care unit: patient, surgical, and anesthetic factors. Anesthesiology. 1994;81:410–8.
Friesen RH, Alswang M. End-tidal PCO2 monitoring via nasal cannulae in pediatric patients: accuracy and sources of error. J Clin Monit. 1996;12:155–9.
Acknowledgments
The research project would not have occurred without the patient and professional assistance of the nursing staff in the post anaesthesia care unit of Cork University Hospital. This work was funded by PMD Solutions.
Conflict of interest
P.L. has no financial interest in the RespiraSense device or PMD Solutions.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article

Cite this article
Lee, P.J. Clinical evaluation of a novel respiratory rate monitor. J Clin Monit Comput 30, 175–183 (2016). https://doi.org/10.1007/s10877-015-9697-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-015-9697-4