
Abstract
With the ageing population, mobility is an important issue and it deters the elderlies to visit health clinics on a regular basis. Individuals with disabilities also face the same obstacles for their out-of-home medical visits. In addition, people living in remote areas often do not get the needed health care attention unless they are willing to spend the time, effort and cost to travel. Advances in information and telecommunication technologies have made telemedicine possible. Using the latest sensor technologies, a person’s vital data can be collected in a smart home environment. The bio-information can then be transferred wirelessly or via the Internet to medical databases and the healthcare professionals. Using the appropriate sensing apparatus at a smart home setting, patients, elderlies and people with disabilities can have their health signals and information examined on a real-time and archival basis. Recovery process can be charted on a regular basis. Remote emergency alerts can be intercepted and responded quickly. Health deterioration can be monitored closely enabling corrective actions. Medical practitioners can therefore provide the necessary health-related services to more people. This paper surveys and compiles the state-of-the-art smart home technologies and telemedicine systems.
Similar content being viewed by others


1 Introduction
In the past decade, one of the fastest growing multidisciplinary research areas is telemedicine. Many definitions of this term exist depending on the specific context. Other terms that often used interchangeably, in conjunction with, or under the umbrella of telemedicine, include telehealthcare, telemonitoring, e-health, e-care, ambient assisted living, smart homecare etc. All these terminologies, though, have the same objectives of delivering remote healthcare to an individual’s home and enabling continuous health monitoring and emergency management.
The increasing attention given to telemedicine is due to many factors. With unaccommodating transportation, and crowed hospitals and clinics in most cities, it is difficult for the elderlies and physically challenged to venture out of their homes to meet with health professionals for the needed treatment or for their routine clinical check-ups. Similarly, healthcare delivery in remote rural areas is a demanding endeavour. Having the capability of delivering healthcare services at the patients’ home not only saves a great deal in monetary and human resources, but it also reduces response time in emergency situations. This is especially beneficial in the case where a large number of patients can be dealt with via communication technologies quickly from a centralized location without sending medical personnel to their individual homes.
Telemedicine has drawn worldwide attention in the 2000s as modern technologies have made remote healthcare delivery a reality. Within the European Community, there were the HHH (home or hospital in heart failure) trials of a low-cost, self-managed home monitoring system for patients with chronic heart failures (Pinna et al. 2003). It was found that monthly home telemonitoring of cardiorespiratory signals being sent to a centralized interactive voice responding system is feasible and patients’ compliance is high. The SM4All (Smart hoMes for ALL) project initiated by the European commission aims to provide a middleware platform for pervasive embedded service in a smart environment (Baldoni 2009). The objectives of SM4All are to provide dependability, scalability, privacy and security to users with disabilities.
The Brazilian family health program was initiated for preventive medicine delivered to the lower income population living in remote regions (Correia et al. 2008). The associated Borboleta system enables healthcare professionals to use PDAs (personal digital assistants) and mobile communication technologies for providing on-site home healthcare and improving the quality of public health services.
In the USA, healthcare is a big financial burden for government, employers, and citizens. White et al. (2006) discussed major challenges to improve healthcare quality and concluded that a distributed diagnosis and home healthcare paradigm is the best approach for affordability and quality.
Germany has an initiative to provide encrypted health data for patients during emergency using electronic health card (Dunnebeil et al. 2011), though there is resistance by some medical professionals mainly due to privacy issues.
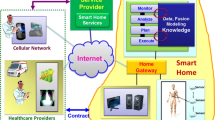
Telemedicine is a multidisciplinary research and application area using advanced technologies in information processing, telecommunication, bio-sensing, and artificial intelligence. Specifically, smart environment and technologies play important roles in making home telemedicine feasible. One can view sensors being the foundation and communication networks as the pillars of a building, supporting various telemedicine applications under the roof to facilitate and provide a smart home environment to individuals, as shown in Fig. 1.

A smart home environment enabling technologies
This work presents a survey of the latest advances in smart environment and home telemedicine. It is an extensively updated version of an earlier work on home telemedicine review (Li and Li 2011). In addition, the current focus is on smart environment and emergency management. There exist numerous works in the literature and therefore only representative, technologically innovative, and interesting systems and approaches are presented. To properly introduce smart environment in telemedicine and emergency management, the fundamental technologies, potential applications, their evaluations, and future directions are presented in a sequential coherent perspective. Section 2 introduces smart environment enabling technologies including communication, sensor and sensor network. Applications of smart telemedicine technologies for specific diseases, emergency management, and the elderly and physically challenged, are presented in Sect. 3. Target user groups’ concerns and healthcare professionals’ evaluation of telemedicine and smart homecare systems are discussed in Sect. 4. In the concluding Sect. 5, challenges, concerns and issues related to smart homecare are considered, and future trends of smart homecare environment are identified.
2 Enabling technologies for smart home telemedicine environment
In order to provide telemedicine effectively, various techniques and methodologies from different areas have to be integrated seamlessly into a smart system. This section examines the primary state-of-the-art enabling technologies for smart environment within a homecare setting for telemedicine: communication and associated telehealth standards, sensors, and sensor networks.
2.1 Communication technology
Many telemedicine systems leverage the latest mobile and wireless communication technologies as well as the widely available internet infrastructure to deliver quality services to home patients (Castro et al. 2001; Bonacina and Masseroli 2006; Li et al. 2008). A home patient monitoring system proposed by Figueredo and Dias (2004) uses a simple RS232 serial interface to connect a mobile phone to patient monitoring devices, and transmits vital signs over the internet to the hospital. vNurse is a system developed by Rehunathan et al. (2011) that uses the smart phone platform to provide secure and remote patient monitoring. Bio-data in vNurse are collected from a wireless body network and transmitted using mobile networks with IP (internet protocol) connection.
Multi-agent systems are commonly found in smart telehealth applications. One of the earliest telemedicine projects, the independent lifestyle assistant, incorporates techniques in sensing model, distress situation detection, network response planning and machine learning (Haigh et al. 2002). The Assistant is implemented as a multi-agent oriented assistive living architecture. Liao et al. (2009) presented a telemonitoring architecture based on mobile agents and they also addressed the issues of reliability, security, and manageability of this platform.
Bramanti et al. (2010) employed GIS (geographical information system) technology to identify the optimal locations of clinics that could provide neurological telemedicine services to patients. A remote-client, service-center architecture was proposed that uses 3G/CDMA network and the internet to transfer vital sign information and medical analysis reports (Zhang et al. 2010).
The web is a common and well-developed medium for communicating monitored and emergency data. Raad and Yang (2009) used the web for reporting real-time status and actions of a home bound elderly. Voice over IP (VoIP) is another family of technologies and communication protocols that can be used effectively in smart environment and telehealthcare. Menkens and Kurschl (2010) investigated and evaluated VoIP enabled communication platforms and proposed a system for regular monitoring as well as providing responsive actions in emergency situations.
Citing decision and notification delays in typical telemedicine homecare settings, as a result of the large volume of information occupying the limited communication resources and consuming valuable computation resources on the remote server, Chen (2010) team designed a smart gateway bridging a home-based wireless senor network and a public communication network. Implemented as a standalone embedded system, the gateway is also capable of tracking a patient’s health state and providing fast response in emergencies.
2.1.1 Telemedicine communication standards
Communication is the foundation of providing telehealthcare in the smart home environment. There are many existing and emerging standards such as the IHE (integrating the healthcare enterprise) recommendations for information exchange (IHE 2012), and the very popular Zigbee (Zigbee Alliance 2012) that have been used in many smart environment projects (Lin and Sheng 2008; Fraile et al. 2010).
de Toledo et al. (2006a, b) argued that in order for e-health to progress, the use of standards in providing plug-and-play devices and interoperable modules is necessary. ISO/IEC 29341 universal plug and play (UPnP) device architecture (ISO 2012a) is a standard for plug-and-play. Lin and Sheng (2008) carried out a study of using UPnP network protocols to facilitate services in a residential network. Park et al. (2011) examined the ISO/IEEE 11073 point-of-care medical device communication (ISO 2012b) and its compatibility to legacy devices.
One of the important works related to standards is Anagnostaki et al. (2002) development of a codification scheme for vital signs in health information interchange. They also discussed the practical aspect of integrating the proposed scheme into medical devices.
Jang et al. (2007) provided a noteworthy comparison of the key features, including power, complexity, number of nodes, latency, range, expandability, data rate, security, and audio connection, among the short-range communication protocols: Wi-Fi IEEE 802.11b standard (IEEE 2012), ZigBee (ZigBee Alliance 2012), and Bluetooth (Bluetooth 2012). Ultra-wideband radio has also been proven to be effective in a smart home environment (Bonato 2010).
2.2 Sensor technology and network
Many research projects have drafted an exhaustive list of sensors to be used in their prototype work such as the TAFETA (technology assisted friendly environment for the third age) group’s implementation (Arcelus et al. 2007). TAFETA has shown how various sensors can be used effectively for different purposes in a smart home: magnetic switches on doors to monitor entry and exit, thermistor to track temperature, accelerometers on chairs and flooring to measure impact which is indicative of a falling condition, RFID (radio-frequency identification) to assist people with Alzheimer or dementia, infrared motion sensor to detect mobility and presence, microphone array to detect abnormal noises and cries for help, smart grab bars with pressure sensors embedded to measure strength and balance trend, and pressure sensitive mats under bed to monitor deviated entry and exit patterns.
In a typical smart home telemedicine system, there are two major types of data that need to be collected. The occupant’s health state and the environmental information are important parameters to monitor and track. Different types of sensors can be used to detect vital signs such as ECG (electrocardiogram) for heart rate, EMG (electromyogram) for muscle activities, and blood pressure monitor for hypertension, while accelerometer, microphone, light sensor, air pressure recorder, and humidity indicator can be used to detect motion and location (Fraile et al. 2010). In addition to signals obtained from sensors that are attached to the body or physical measurement devices in the home, there are other media that could be monitored such as video and sound. Though, sound is the preferred medium due to privacy concerns.
Istrate et al. (2006) team developed a sound analysis system to detect and classify alarming sounds in a noisy environment. Using wavelet technology to process sound signals, their system achieves good performance comparable to other systems using different monitoring technologies. Laydrus et al. (2007) investigated the use of frequency domain features in an automated sound analysis system and was able to achieve over 90 % accuracy in classifying 19 real-world sounds. Vacher et al. (2009) presented a sound classification and speech recognition system with microphones placed in the home to detect short sentences or words that may indicate a distress situation. Though, Fleury et al. (2008) found that screams and distress sentences are difficult to differentiate due to distress sentences are similar to short words. Hollosi et al. (2010) devised an acoustic event detection and classification system for ambient assistive living environment and interpreted coughing as an indicator of upcoming illness.
Pressure sensors have been used extensively in various parts of a smart home. Arcelus et al. (2009) installed pressure sensors under the bed and on the floor next to the bed. Their collected data include sitting pressure, standing pressure, and the time from sit to stand, which provide valuable information on a patient’s mobility and other health-related data. Leusmann et al. (2011) used arrays of Piezo sensors to implement a sensor floor to track the whereabouts of the home occupants. Moreover, data collected can be used to analyze impact patterns in case of fall or other emergency situations. Similarly, Miao et al. (2009) proposed a fall detection approach based on head tracking using two video cameras. They constructed three-dimensional head position models with unimportant objects and background filtered out.
Location tracking is an important aspect of providing a smart home environment. Global positioning system (GPS) has limitation operating indoor. Various techniques have been used for indoor position location including the use of cascade correlation network and neural network modeling (Chen et al. 2011). Helal et al. (2003) at the University of Florida has been working on the house of Matilda project for the past several years. Matilda is an in-laboratory mock up house to experiment various innovative ideas for smart home. One of their focuses is location tracking of the elderly by the use of ultrasonic sensor technology.
Wearable devices have been research extensively in the past decade. With the advances in device miniaturization and communication techniques, wearable devices can serve many different roles in telehealthcare, for instance, as a standalone monitoring device or as a node in a sensor network (Hung et al. 2004; Axisa et al. 2005; Kang et al. 2006). Chaczko et al. (2008) developed a small wearable device that incorporates data storage, display screen, speaker, microphone, GPS, RFID and accelerometers. The ability to monitor and locate makes this an ideal device to be installed in various places in the home and on the patient. Wang et al. (2007) presented a body piconet based on smart sensor nodes for ECG. Their work uses Bluetooth technology for in-home data transfer and the internet for network data transfer to a hospital.
Nag and Sharma (2006) presented their work on a wireless smart clothing system that is capable of acquiring ECG, pulse oximetry, body motion/tilt and skin temperature data. Bonato (2010) gave an extensive survey and review of the major approaches to implement wearable systems. Enabling technologies discussed in that work include miniaturization, lower-power radio, and dedicated operating system, which make body sensor network a reality.
Instead of focusing on specific or a few signals, multimodal systems are gaining popularity. Medjahed et al. (2009) presented a fuzzy logic system utilising a wide range of sensors to recognize activities in a home environment. These sensors include physiological types (cardiac frequency, activity, agitation, posture and fall detection), microphones, infrared, water debit and state-change in appliances.
Many innovative and non-intrusive approaches have been developed in the past several years. Ichihashi and Sankai (2007) developed a small ‘smart telecom’ unit that integrates sensing circuit, digital signal processor, and wireless communication into a device of size 25 by 37 mm. Such small devices can monitor one’s vital signs without being invasive. Kim et al. (2007) developed an integrated home health monitor using a chair as a non-invasive platform. This all-in-one monitor can record ECG, estimate blood pressure, measure blood glucose level and ear temperature. These sampled signals are then transmitted to a home server using Zigbee technology, which in turn are transmitted to a healthcare center via the internet.
Ho et al. (2009) presented a very interesting initiative in an attempt to harvest body temperature and vibrations in the house to power implantable glucose sensors within a wireless home network. Ping et al. (2009) home healthcare research project places heavy emphasis on recognizing a patient’s emotional state in addition to physical state. Facial, vocal, eye-movement, and physiological signals are tracked and analyzed to provide the psychological aspects of a patient’s health.
Hussain and colleagues (2009) explored the integration of RFID and wireless sensor network in a smart home environment. Their idea is to use the wireless sensor network for tracking the movement and location of individuals while the identification of a person can be accomplished by the wearing of RFID tags. The separation of these events allows for quick decision-making and responses to various situations.
3 Smart telemedicine applications
This section presents the major application areas that smart telemedicine plays a dominant role.
3.1 Smart diagnostics systems for specific diseases
Unlike face-to-face medical consultation, useful information must be derived from the raw data in telemedicine. It is almost impossible for humans to examine this large volume of data manually and to detect any changes. Therefore, techniques have to be developed in order to automate the diagnostics and abnormality detection process. This section introduces smart telehealth systems developed for specific illnesses.
Back in 2000, Finkelstein and Friedman (2000) presented a home asthma telemonitoring system that has the capability of assisting asthma patients in self-care plans as well as alerting healthcare personnel when distress situation is detected. Lau et al. (2002) implemented a multimedia system that employs bio-sensor data, messages and video transmission to allow physicians and patients with shoulder replacement surgery to communicate and monitor the progress. Chun et al. (2003) developed a home telemedicine system for cardiac and respiratory disease, diabetes, and hypertension. Using artificial intelligence techniques, this system is capable of providing automated diagnostic and consultation. Performance evaluation has shown that the implemented system is a viable alternative to personal monitoring and consultation.
Rudi and Celler (2006) presented an expert telemedicine system that is capable of storing various data and measurement related to diabetes management. In addition to present to medical professionals records associated with individual patients, the system is also capable of recommending insulin dose adjustment to patients. Jiang and Xie (2009) proposed a telehealth monitoring system that uses data mining techniques to deal with the large volume of biological data. They also utilized association rules to recommend actions to be taken for hypertension. Zhang et al. (2009) developed a chronic disease management system using a real-time knowledge base and the case based reasoning approach, together with a web patient monitoring system, to improve the diagnostic of diabetes and hypertension.
Fergus et al. (2009) developed a body area sensor network intended for physiotherapist’s use. This system collects and stores motion data of the home patient, and provides some quantitative assessments of the patient’s progress. Gobbi et al. (2009) designed a system that addresses issues related to real-time data processing, network architecture, and web-based data management and services. As an automated home monitoring system for lung obstruction, that system was shown to be reliable and efficient. Silva et al. (2010) developed an internet-based system for home monitoring of patients with respiratory muscle disorders. They concluded that their system would be a useful tool for the evaluation of inspiratory muscle in telemedicine services, thus reducing the costs of handling these patients.
A smart home with technologies to enhance the quality of life of quadriplegia patient was proposed by Uzunay and Bicakci (2007). They placed heavy emphasis on the security aspect of their voice activated smart home facilities. To monitor blood flow velocity in a wireless home environment, Wu et al. (2011) presented a self-monitoring device to measure blood flow velocity that is integrated in a LabVIEW (LabView 2012) mobile environment. Smart home telemedicine technology is ideal for patient self-monitoring and quality of life improvement, which are the subjects in the next section.
3.2 Elderly and assistive technology
The segments of our population that need quality healthcare the most are the elderly and physically impaired. Home telemedicine and telehealthcare systems are the solution to deliver low-cost yet quality services for these individuals.
In 2006, the United Nation estimated that at least 650 million people have disabilities worldwide (United Nation 2006). There are various types and degrees of disabilities. According to the Massachusetts Department of Elementary and Secondary Education, the impairments can be classified into communication, emotional, health, intellectual, neurological, physical, and sensory (MDESE 2000). Andrich et al. (2006) presented their smart home project with case studies involving people with disabilities in different categories: hemiplegia, paraplegia, quadriplegia, motor impairment, and cognitive impairment. Disabled person with the specific type of impairment would require specialised care and tailored smart home technologies.
Many telehealth and assistive systems have been proposed and are in place for the elderlies. Meng et al. (2000) has been working on teleoperated mobile robots via the internet to provide quality healthcare to the elderly. They have also designed robotic pets that are capable of physiological data collection and transmission, as well as simple healthcare tasks (Ling et al. 2005). Briere and colleagues (2009) presented a teleoperated mobile robot with videoconferencing capability for in-home telerehabilitation services.
Vergados et al. (2008, 2010) discussed their INHOME project which goal is to provide intelligent ambient assistive living services to elderly people at home for independent living. Lim et al. (2010) presented a home healthcare set-top box specially designed for the elderlies. Their work focused on standard compatibility and adherence to the ISO/IEEE 11073 personal health data standard. Vinjumur et al. (2010) implemented a web-based medicine management system that uses RFID tags to monitor medication intake for the elderly at home.
With multimodal signal sampling, it is imperative to incorporate data fusion techniques in telehealth monitoring and decision-making. Virone et al. (2003) investigated data fusion of collected video and sound signals in the monitoring of elderly patients at home. Medjahed’s group focused on data fusion of multi-senor inputs to provide medical recommendation using a rule based approach (Medjahed et al. 2011).
Artificial intelligence techniques play a major role in smart home systems. Papamatthaiakis and colleagues (2010) presented an indoor activity recognition system for the elderlies. Using association rules and Allen’s temporal relations, they claimed a 100 % recognition rate in identifying everyday activity such as bathing, preparing meals, doing laundry, etc. The MavHome project aims to provide a smart and adaptive environment for inhabitants (Jakkula et al. 2007). In order to meet the goals of comfort and efficiency in MavHome, health trend monitoring and prediction are made using support vector machine and forecasting tools based on time series data collected in a sensor network. Huo et al. (2009) presented a healthcare environment for the elderlies using a home sensor network and a body sensor network. The interesting aspects of this work lie in the functionalities provided, including outdoor monitoring, and emergency decision and alarms. Various communication techniques, such as automated telephone call, SMS and email, are integrated into the system, transmitting emergency signals to caregivers and family members. Smart decision-making using hidden Markov model is proposed to speed up the decision process, increase the accuracy of event detection, minimise measurement errors, and correct transmission errors.
Franco et al. (2010) proposed the use of passive infrared sensors placed in the living quarters of an elderly person to detect abnormal changes in behavior. This system would allow early admission of dependent care for those who show a shift in daily routine, for example, individuals with Alzheimer disease. The monitoring of behavioural changes is an area of interest in telehealth since the onset of certain alarming situations could be detected and healthcare professionals could then be notified. The next section focuses on using smart healthcare system to handle emergency.
3.3 Emergency planning and management
Emergency planning and management with respect to in-home healthcare has been a vigorously research topic. Rosen et al. (2002) proposed the Cybercare system to handle national scale disasters. Taking a military approach to map strategy, operations and technology to the healthcare realm of policy, functionality and network infrastructure technologies, they argued the necessity of a nation-wide support information infrastructure to cope with disaster, and of incorporating surge-capacity into a national disaster response system.
Citing the fact that the patients who receive critical emergency services often are not the actual victims of the disaster or outbreak such as SARS (severe acute respiratory syndrome), Joseph et al. (2005) developed a home healthcare disaster planning, recovery, and management system to facilitate treatment of the actual victims. By integrating in-home intelligent devices to provide timely measured information to public offices such as Red Cross, local police etc., they reasoned that the medical personnel can provide homecare remotely and deal with a mass-scale epidemic and natural disasters appropriately.
Smart environment not only can be used in a home environment but can also be used outdoor. Smalls et al. (2009) devised a health monitoring system for use in mass causality emergency situations. By placing a health monitoring device on the body of a victim and integrating this node to a wireless ad-hoc network, vital signs of the victim can be transmitted to regional and national emergency response institutions. This is particular useful in cases where infrastructures are non-operational due to catastrophic disaster or when communication channels are overwhelmed by emergency requests. Advances in wireless technology have driven down the cost of ad-hoc networks, and with fewer attending field personnel, Smalls et al.’s approach may prove to be cost effective in the very near future. Wouhaybi et al. (2010) also proposed a system with similar objectives but they focused on the reduction of false alarm using a rule-based decision system. A disaster management framework proposed by Bessis et al. (2010) integrates various technologies including web services, grid and cloud computing, ad-hoc mobile networks, and wearable and body sensors. Their aim is to provide coherent and collective resource utilization and decision-making for multiple parties in emergency situations.
Jang et al. (2007) proposed a system using multiple sensor technologies including bio-sensors to monitor an elderly’s daily physiological status. Many services are provided to the patient including early warning due to a change of health status, advice for health improvement, and appointment with specific medical practitioners. In addition to sensors, an active robot that provides services to human is part of a smart assistive environment proposed by Lin et al. (2009). Using multimodal observations to recognize voice and other events, their project shows that health predictions, evaluations, and decisions become more reasonable in the evaluation of emergency level and the assistance required in critical events.
4 Smart environment and telemedicine system evaluation
In one of the early studies, de Lunsignan et al. (2000) examined the effectiveness of a home cardiopulmonary monitoring system. This system collects various vital measures via sensors attached to the body and transmits the data wirelessly to a nearby unit at the patient’s home. The data are then transferred to a centralised monitoring station. They found the system is acceptable to patients, functionally satisfactory in the home environment, and very reliable in the collection of objective data.
Capomolla et al. (2004) monitored patients with CHF (chronic heart failure) either under usual care or telemonitoring care. Their study showed that home telemonitoring is more effective than usual care in reducing healthcare requirements and can improve outcome in CHF patients. Raju et al. (2004) presented their study on the cost effectiveness of mobile telemedicine applications, and the quality of care and medical error reduction. They reported on their extensive literature search and felt that the findings are inconclusive and well-designed protocols are necessary to conduct further large-scale investigations.
Zhang and Bai (2005) used a queueing model to evaluate the performance of a home ECG and blood pressure monitoring system based on trial data over a 4-month period. Their objective was to study the traffic load, response time, and scalability of the system. The results are more than satisfactory and show great potential of the examined monitoring system. de Toledo et al. (2006a) reported their experience in using a telemedicine homecare system for patients with chronic obstructive pulmonary disease. Their results suggest that home telemedicine services provide good support to the healthcare professionals, improve patients’ condition, and incur low costs.
Jasemian (2008) argued that a successful telemedicine application depends on the patient’s compliance, trust and comfort in such home-based systems. An experiment was carried out in 2008 with the patients using ECG monitoring device with a real-time wireless system continuously for a long period of time. Over half of the participants found the system user friendly, reliable, and usable with acceptable performance. Though they found the ECG device heavy and not user-friendly.
Some have argued that the evaluation of home telehealth information systems should not be assessed simply on grounds of technical innovation but should use a holistic interpretive approach. In 2008, Kaldoudi and colleagues (2008) proposed a framework for evaluating home telehealth intervention, together with its application for peritoneal dialysis at home.
Ojasalo et al. (2010) conducted a study on smart home technologies and services for intellectually disabled. They found that safety technologies are very well received, and the balance of safety and privacy can be addressed by the appropriate technologies. A 2011 study conducted by Ziefle et al. (2011) on the acceptance of video monitoring in smart home environment for elderly and disabled reveals that acceptance and users’ needs and wants are the main issues in a successful deployment of such home medical monitoring technology. The study also shows that there are serious concerns that data may be altered, illegally accessed, and deleted intentionally or due to system failure or virus attack.
Beer and Takayama (2011) performed a study on elderlies who used a mobile remote presence (MRP) system. This study reveals many interesting issues. Benefits of MRP identified by the elderlies include being able to see and be seen with a MRP system, reduction in travel costs and hassles, and a decrease in isolation in a social context. However, concerns raised include MRP usage etiquette, personal privacy, possible overuse, and reliance on the system. Though the elderlies in the study are not technologically inclined, they prefer to operate the MRP system by themselves.
5 The future of telemedicine
Smart home healthcare and telemedicine systems are here to stay, but there are still many challenges and issues to be resolved. Innovation is important to improve the efficiency and effectiveness, and hence acceptance, of these systems.
5.1 Challenges and issues
Security is major concern in the acceptance of homecare with modern technologies. Many research groups have focused on one of the most important issue in telemedicine, that of the integrity and security of transmitted data. Simpson et al. (2006) posed several challenging issues regarding continuous home monitoring: who should receive information as the patient, family members, caregivers and medical professionals all have interest; what information should each person receive without violating any data privacy and security concerns; how should information be presented since each party may prefer different mode of communication such as telephone, computer, etc. Proposed solutions to the security issue include cryptography (Mantas et al. 2009) and context-aware access control rules (Guennoun and El-Khatib 2009).
Due to the sensitive nature of health information, privacy is an important issue in data transmission and storage in telehealth systems. Without proper and established protocols and regulations in place, telemedicine would not be used widely as many people are concerned with the privacy of their health information. Kotz and colleagues (2009) compared existing privacy frameworks, identified a set of desirable privacy properties in mobile healthcare systems, and used their findings to propose a privacy framework. They also raised several privacy issues and questions that need to be addressed by technical people, governmental agencies and regulatory organisations.
Reliability is another critical factor in the implementation of smart homecare. Wireless technologies make telehealth care possible, however, such networks that operate in hostile outdoor environment have many reliability issues. Using rural China as a case study, Fong and Pecht (2010) identified and reviewed the factors that can impact on the reliability of telehealth care networks: physical obstacles, atmospheric absorption, inadequate fade margin and system failure.
Gaddam et al. (2008) studied extensively the various issues related to the implementation of sensor networks for home healthcare and emergency. They have identified potential challenges including interoperability and interference, real-time data acquisition and processing, reliability and robustness, energy conservation, data management, data privacy and security, and comfort and unobtrusive operation. In addition, design issues for wireless networks considered are deployment of sensor nodes, mobility of wireless sensor, cost and size of the wireless node, infrastructure of the network, network coverage, network size, power management, life-time of the sensor networks, and quality of service requirements in such networks.
5.2 Innovation and trends
Since the second-half of the 2000s, there have been numerous reported work and innovation in smart healthcare systems. Taylor and Dajani (2008) gave a sound argument that the future home healthcare systems should take into consideration a well-balanced implementation infrastructure based on the web, mobile, and broadband technologies. Moritz et al. (2009) emphasized the importance of various fundamental issues in using interoperable devices in home healthcare. These issues include energy consumption, power supply, memory, computing power, and bandwidth.
Koufi and colleagues (2010) implemented a grid portal that provides services to people who need medical advice at their homes. The portal is an integrated system of wireless personal digital assistants (PDAs) and grid technology, with heavy design emphasis placed on security access and storage of data.
For telehealth, the monitoring of an individual creates a continuous stream of data that must be stored either locally at home or at a centralised database. Lasierra et al. (2010, 2011) used an ontology approach to arrange patient data and records in a formal structure so as to support health information interoperability.
Invasive devices are being recognised as one of the prime reasons at-home patients are hesitant to use telehealth care monitoring systems. Motoi et al. (2010) demonstrated the possibility of using non-invasive technologies for home healthcare. Devices are installed on toilets, bathtubs, and beds to measure various vital signals. They deployed this prototyping system for subjects with cardiovascular disease or sleep disorder successfully.
Modifying and conditioning patient’s behaviour is another innovative trend that is gaining attention these days. Evers and Krose (2010) developed a monitoring system tracking the physical and emotional condition via a sensor network. Patients are provided with feedback to promote activities and behaviour with positive health impact. Also, the integration of wearable technology and robots is a promising avenue to facilitate therapeutic intervention for chronic conditions, which potentially can reap benefits from these combined technologies (Bonato 2010).
Point-of-care testing is another developing trend in enhancing home healthcare. Many innovative devices are being investigated that potentially shorten the time between testing and diagnostic, and are especially useful in rural settings. Beyette et al. (2011) provided a comprehensive survey and a special volume on these innovative handheld and home-based devices. These devices include sensors for multispectral imaging, tomography, cardiac, EEG, Chlamydia trachomatis, bladder pressure, respiratory impairment, as well as for detection and analysis of macula swelling, pathogen detection, metabolic syndrome prediction, energy metabolism, Chagas disease, vascular tree identification, Parkinson’s disease, etc.
Back in 2005, Stankovic et al. (2005) at the University of Virginia identified three critical development issues in wireless sensor networks for in-home healthcare. The first issue is the enabling technologies for future medical devices: interoperability, real-time data acquisition and analysis, reliability and robustness, and new node architectures. Embedded, real-time, networked system infrastructure is the other critical development area which includes patient and object tracking, communication, interference, multimodal collaboration, energy conservation, and multi-tiered data management. The third issue concerns medical practice-driven models and requirements including role-base access control and delegation in real-time, unobtrusive operation, and records and data privacy and security.
The critical development areas of concern, as suggested by Stankovic’s team, have not yet been fully addressed with today’s technology. There are ample opportunities for research and development in improving telemedicine systems as they are still at an infancy stage. Some of the challenges and issues in building a smart home environment are shown in Fig. 2. Without a doubt, smart home telemedicine systems will be deployed in an increasingly rapid pace in the years to come.

Challenges and issues in building smart home
References
Anagnostaki A et al (2002) A novel codification scheme based on the VITAL and DICOM standards for telemedicine applications. IEEE Trans Biomed Eng 49(12):1399–1411
Andrich R et al (2006) The DAT project: a smart home environment for people with disabilities. In: 10th international conference on computers helping people with special needs, ICCHP, Austria, July 2006, pp 492–499
Arcelus A et al (2007) Integration of smart home technologies in a health monitoring sysem for the elderly. In: 21st international conference on advanced information networking and applications workshops, IEEE, Canada, pp 820–825
Arcelus A et al (2009) Determination of sit-to-stand transfer duration using bed and floor pressure sequences. IEEE Trans Biomed Eng 56(10):2485–2492
Axisa F et al (2005) Flexible technologies and smart clothing for citizen medicine, home healthcare, and disease prevention. IEEE Trans Info Technol Biomed 9(3):325–336
Baldoni R et al (2009) An embedded middleware platform for pervasive and immersive environments for-all. In: IEEE communications society conference on sensor, Mesh and Ad Hoc Communications and Networks, Rome, pp 1–3
Beer JM, Takayama L (2011) Mobile remote presence systems for older adults: acceptance, benefits, and concerns. In: International conference on pervasive technologies related to assistive environments, pp 19–26
Bessis N et al (2010) The big picture, from grids and clouds to crowds: a data collective computational intelligence case proposal for managing disasters. In: 5th IEEE international conference on P2P, parallel, grid, cloud and internet computing (3PGCIC-2010), Fukuoka, 4–6 Nov 2010, ISBN: 978-0-7695-4237-9, pp 351–356
Beyette FR et al (2011) Point-of-care technologies for health care. Special issue IEEE transactions on biomedical engineering, 58(3):732–735
Bluetooth (2012) The bluetooth special interest group. http://www.bluetooth.com. Accessed 13 Jan 2012
Bonacina S, Masseroli M (2006) A web application for managing data of cardiovascular risk patents. In: International conference on engineering in medicine and biology society, pp 6324–6327
Bonato P (2010) Wearable Sensors and Systems. IEEE Eng Med Biol Mag 29(3):25–36
Bramanti A et al (2010) GIS and spatial analysis for costs and services optimization in neurological telemedicine. International conference on engineering in medicine and biology society, pp 2204–2207
Briere S, Boissy P, Michaud F (2009) In-home telehealth clinical interaction using a robot. In: Proceedings of the 4th ACM/IEEE international conference on human-robot interaction, La Jolla, 09–13 Mar 2009, pp 225–226
Capomolla S et al (2004) Heart failure case disease management program: a pilot study of home telemonitoring versus usual care. Eur Heart J Suppl 6(F):F91–F98
Castro D et al (2001) Patient Telemonitoring at Home engineering in medicine and biology society. In: Proceedings of the 23rd annual international conference of the IEEE, pp 3571–3574
Chaczko Z et al (2008) Applications of cooperative WSN in homecare systems. In: International conference on broadband communications, information technology and biomedical applications, pp 215–220
Chen RC et al (2011) Indoor position location based on cascade correlation networks. In: IEEE international conference on systems, man, and cybernetics, 9–12 Oct 2011, pp 2295–2300
Chen Y et al (2010) A smart gateway for health care system using wireless sensor network. In: International conference on sensor technologies and applications, pp 545–550
Chun H et al (2003) Development of an integrated home telemedicine system. In: IEEE asian-pacific conference on biomedical engineering, Nara, 20–22 Oct 2003, pp 46–47
Correia R et al (2008) Borboleta: a mobile telehealth system for primary homecare. In: Proceedings of ACM symposium on applied computing, Ceara, 16–20 Mar 2008, pp 1343–1347
de Lunsignan S et al (2000) A pilot study of radiotelemetry for continuous cardiopulmonary monitoring of patients at home. J Telemed Telecare 6(1):119–122
de Toledo P et al (2006a) Telemedicine experience for chronic care in COPD. IEEE Trans Info Technol Biomed 10(3):567–573
de Toledo P et al (2006b) Towards e-health device interoperability: the Spanish experience in the telemedicine research network. In: Proceedings of international conference on engineering in medicine and biology society, pp 3258–3261
Dunnebeil S et al (2011) Encrypted NFC emergency tags based on the German telematics infrastructure. In: 3rd international workshop on near field communication, 22 Feb 2011, pp 50–55
Evers V, Krose B (2010) Toward an ambient empathic health companion for self care in the intelligent home. In: Annual European conference on cognitive ergonomics, pp 365–366
Fergus P et al (2009) remote physiotherapy treatments using wireless body sensor networks. In: International wireless communications and mobile computing conference, pp 1191–1197
Figueredo M, Dias J (2004) Mobile telemedicine system for home care and patient monitoring. In: IEEE international conference on engineering in medicine and biology society, pp V1-3387–3390
Finkelstein J, Friedman RH (2000) Home asthma telemonitoring (HAT) system. Chest 117(1):103–104
Fleury A et al (2008) Sound and speech detection and classification in a health smart home. In: IEEE international conference on engineering in medicine and biology society, pp 4644–4647
Fong B, Pecht MG (2010) Prognostics in wireless telecare networks: a perspective on serving the rural Chinese population. In: Prognostics and health management conference, pp 1–6
Fraile JA et al (2010) Applying wearable solutions in dependent environments. IEEE Trans Info Technol Biomed, 14(6):1459–1467
Franco C et al (2010) Behavioral telemonitoring of the elderly at home. In: IEEE conference on advanced information networking and applications workshops, pp 759–766
Gaddam A et al (2008) Wireless sensors networks based monitoring: review, challenges and implementation issues. In: International conference on sensing technology, pp 533–538
Gobbi A et al (2009) A new telemedicine system for the home monitoring of lung function in patients with obstructive respiratory diseases. In: International conference on e-health, telemedicine, and social medicine, pp 117–122
Guennoun M, El-Khatib K (2009) Securing medical data in smart homes. In: International workshop on medical measurements and applications, pp 104–107
Haigh KZ et al (2002) An open agent architecture for assisting elder independence. In: International joint conference on autonomous agents and multi-agent systems, pp 578–586
Helal S et al (2003) Enabling location-aware pervasive computing applications for the elderly. In: IEEE international conference on pervasive computing and communications, pp 531–536
Ho C et al (2009) Technologies for an autonomous wireless home healthcare system. In: International workshop on wearable and implantable body sensor networks, pp 29–34
Hollosi D et al (2010) Voice activity detection driven acoustic event classification for monitoring in smart homes. In: International symposium on applied sciences in biomedical and communication technologies, pp 1–5
Hung K et al (2004) Wearable medical devices for tele-home healthcare. In: International conference on engineering in medicine and biology society, pp 5384–5387
Huo H et al (2009) An elderly health care system using wireless sensor networks at home. In: International conference on sensor technologies and applications, pp 158–163
Hussain S, Shaffner S, Moseychuck D (2009) Applications of wirelesssensor networks and RFID in a smart home environment. In: Annual communication networks and services research conference, pp 153–157
Ichihashi F, Sankai Y (2007) Development of a portable vital sensing system for home telemedicine. In: International conference on engineering in medicine and biology society, pp 5872–5877
IEEE 802.11 (2012) Wireless local area networks standard. Institute of Electrical and Electronics Engineers. http://standards.ieee.org/about/get/802/802.11.html. Accessed 13 Jan 2012
IHE (2012) Initiative by healthcare professionals. http://www.ihe.net. Accessed 13 Jan 2012
ISO/IEC 29341 (2012a) UPnP universal plug and play standared. Internatioal Organization for Standardization. http://www.iso.org/iso/iso_catalogue/catalogue_tc/catalogue_detail.htm?csnumber=52676. Accessed 13 Jan 2012
ISO/IEEE 11073 (2012b) POC device communication standard. International Organization for Standardization. http://www.iso.org/iso/iso_catalogue/catalogue_tc/catalogue_detail.htm?csnumber=37890. Accessed 13 Jan 2012
Istrate D et al (2006) Information extraction from sound for medical telemonitoring. IEEE Trans Info Technol Biomed 10(2):264–274
Jakkula VR, Cook DJ, Jain G (2007) Prediction models for a smart home based health care system. In: International conference on advanced information networking and application workshops, pp 761–765
Jang S-J et al (2007) Ubiquitous home healthcare management system with early warning reporting. In: International conference on convergence information technology, pp 2394–2401
Jasemian Y (2008) Elderly comfort and compliance to modern telemedicine system at home. In: International conference on pervasive computing technologies for healthcare, pp 60–63
Jiang X, Xie C (2009) Home health telemonitoring system based on data mining. In: International forum on information technology and applications, pp 431–434
Joseph VC et al (2005) Intelligent healthcare systems: re-defining personal healthcare solutons. In: International conference on advanced communication technology, pp 424–427
Kaldoudi E, Chatzopoulou A, Vargemezis V (2008) An interpretive approach in the evaluation of homecare telematics interventions. In: PETRA 2009 2nd international conference on pervasive technologies related to assistive environments, Corfu, 9–13 Jun 2009
Kang TH et al (2006) Sensors on textile substrates for home-based healthcare monitoring. In: Distributed diagnosis and home healthcare conference, pp 5–7
Kim JS et al (2007) Development of HIHM (home integrated health monitor) for ubiquitous home healthcare. In: International conference on engineering in medicine and biology society, pp 363–365
Kotz D, Avancha S, Baxi A (2009) A privacy framework for mobile health and home-care systems. In: ACM workshop on security and privacy in medical and home-care systems, pp 1–12
Koufi V, Malamateniou F, Vassilacopoulos G (2010) A system for the provision of medical diagnostic and treatment advice in home care environment. J Adv Pervasive Ubiquitous Comput 14(6):551–561
LabView (2012) National instruments. http://www.ni.com/labview. Accessed 13 Jan 2012
Lasierra N et al (2010) An ontology approach to manage individual patient profiles in home-based telemonitoring scenarios. In: IEEE international conference on information technology and applications in biomedicines, pp 1–4
Lasierra N et al (2011) Home-based telemonitoring architecture to manage health information based on ontology solutions. In: IEEE international conference on information technology and applications in biomedicines, pp 1–4
Lau C et al (2002) Asynchronous web-based patient-centered home telemedicine system. IEEE Trans Biomed Eng 49(12):1452–1462
Laydrus NC et al (2007) Automated sound analysis system for home telemonitoring using shifted delta cepstral features. In: International conference on digital signal processing, pp 135–138
Leusmann P et al (2011) Your floor knows where you are: sensing and acquisition of movement data. In: International conference on mobile data management, pp 61–66
Li KF, Li W (2011) A survy on home telemedice. In: International conference on broadband and wireless computing, communication and application, pp 472–477
Li X et al (2008) Home healthcare platform based on wireless sensor networks. In: International conference on information technology and application in biomedicine, pp 263–266
Liao J et al (2009) An extensible telemonitoring architecture based on mobile agent method. In: IEEE international conference on robotics and biomimetics, pp 1537–1542
Lim JH et al (2010) Home healthcare set top-box for senior chronic care using ISO/IEEE 11073 PHD standard. In: International conference on engineering in medicine and biology society, pp 216–219
Lin WW, Sheng YH (2008) Using OSGi UPnP and Zigbee to provide a wireless ubiquitous home healthcare environment. In: International conference on mobile ubiquitous computing, systems, services and technologies, pp 268–273
Lin Y et al (2009) Decision making in assistive environments using multimodal observations. In: International conference on pervasive technologies related to assistive environments, pp 1–8
Lin YJ et al (2008) A study of integrating digital health network with UPnP in an elderly nursing home. In: Asia-Pacific computer systems architecture conference, pp 1–7
Ling QH et al (2005) Robotic pet based interactive home healthcare system. In: International conference on advanced intelligent mechatronics, pp 771–776
Mantas G, Lymberropoulos D, Komninos N (2009) Integrity mechanism for ehealth tele-monitoring system in smart home environment. In: IEEE international conference of the IEEE engineering in medicine and biology society, pp 3509–3512
MDESE (2000) Disability definitions and related links. Massachusetts Department of elementary and Secondary Education. http://www.doe.mass.edu/sped/definitions.html. Accessed 13 Jan 2012
Medjahed H et al (2009) Human activities of daily living recognition using fuzzy logic for elderly home monitoring. In: IEEE international conference on fuzzy systems, pp 2001–2006
Medjahed H et al (2011) A pervasive multi-sensor data fusion for smart home healthcare monitoring. In: IEEE international conference on fuzzy systems, pp 1466–1473
Meng M et al (2000) E-service robot in home healthcare. In: International conference on intelligent robot and systems, pp 832–837
Menkens C, Kurschl W (2010) VoIP based telehomecare application kiosk. In: International conference on information technology: new generations, pp 783–790
Miao Y, Naqvi SM, Chambers J (2009) Fall detection in the elderly by head tracking. In: IEEE workshop on statistical signal processing, pp 357–360
Moritz G et al (2009) Web services to improve interoperability of home healthcare devices. In: International conference on pervasive computing technology for healthcare, pp 1–4
Motoi K et al (2010) Development and clinical evaluation of a home healthcare system measuring in toilet, bathtub and bed without attachment of any biological sensors. In: IEEE international conference on information technology and applications in biomedicine, pp 1–4
Nag S, Sharma DK (2006) Wireless e-jacket for multiparameter biophysical monitoring and telemedicine applications. In: IEEE international summer school on medical devices and biosensors, pp 40–44
Ojasalo J et al (2010) Better technologies and services for smart homes of disabled people: empirical findings from an explorative study among intellectually disabled. In: International conference on software technology and engineering, pp V1-251–259
Papamatthaiakis G, Polyzos GC, Xylomenos G (2010) Monitoring and modeling simple everyday activities of the elderly at home. In: IEEE consumer communications and networking conference, pp 1–5
Park CY et al (2011) ISO/IEEE 11073 PHD standardization of legacy healthcare device for home healthcare services. In: IEE international conference on consumer electronics, pp 547–548
Ping A et al (2009) Designing an emotional majormodo in smart home healthcare. In: International Asia symposium on intelligent interaction and affective computing, pp 45–47
Pinna GD et al (2003) Home telemonitoring of respiratory activity and heart rate variability in chronic heart failure patients: the challenge of the home or hospital in heart failure project. In: IEEE conference on computers in cardiology, pp 197–200
Raad MW, Yang LT (2009) A ubiquitous smart home for the elderly. Inf Syst Frontiers 11(5):529–536
Raju N et al (2004) Status of mobile computing in health care: an evidence study. In: IEEE international conference on engineering in medicine and biology, pp 3274–3277
Rehunathan D et al (2011) vNurse: using virtualisation on mobile phones for remote health monitoring. In: IEEE international conference on e-health networking applications and services, pp 82–85
Rosen J et al (2002) The future of command and control for disaster response. IEEE Eng Med Biol Magazine 21(5):56–68
Rudi R, Celler BG (2006) Design and implementation of expert-telemedicine system for diabetes management at home. In: International conference on biomedical and pharmaceutical engineering, pp 595–599
Silva EP Jr et al (2010) An internet-based system for home monitoring of respiratory muscle disorders. In: IEEE international conference on engineering in medicine and biology, pp 5492–5495
Simpson R et al (2006) Plans and planning in smart homes in LNCS in computer science. Augusto JC, Nugent CD (eds) Designing smart homes, vol 4008, Springer, Berlin, pp 71–84
Smalls J et al (2009) Health monitoring systems for massive emergency situations. In: IEEE long island systems, applications and technology conference, pp 1–11
Stankovic JA et al (2005) Wireless sensor networks for in-home healthcare: potential and challenges. In: Proceedings of the high confidence medical devices, software, and systems workshop
Taylor C, Dajani L (2008) The future of homecare systems in the context of the ubiquitous web and its related mobile technologies. In: Proceedings of the 1st international conference on pervasive technologies related to assistive environments, Athens, pp 1–4
United Nation (2006) Convention on the rights of persons with disabilities, 2006. http://www.un.org/disabilities/default.asp?id=150. Accessed 13 Jan 2012
Uzunay Y, Bicakci K (2007) SHA: a secure voice activated smart home for quadriplegia patients. In: IEEE international conference on bioinformatics and biomedicine workshop, pp 151–158
Vacher M et al (2009) Speech recognition in a smart home: some experiments for telemonitoring. In: Conference on speech technology and human-computer dialogue, pp 1–10
Vergados D et al (2008) Intelligent services for assisting independent living of elderly people at home. In: International conference on pervasive technologies related to assistive environments, pp 1–4
Vergados DD (2010) Service personalization for assistive living in a mobile ambient healthcare-networked environment. J Adv Pervasive Ubiquitous Comput 14(6):575–590
Vinjumur JK et al (2010) Web based medicine intake tracking application. In: International conference on pervasive technologies for assistive environment. Samos, 23–25 Jun 2010
Virone G et al (2003) First steps in data fusion between a multichannel audio acquisition and an information system for home healthcare. In: International conference on engineering in medicine and biology society, pp 1364–1367
Wang D et al (2007) Body piconet for the telemedicine system based on home networks. In: IEEE international conference on complex medical engineering, pp 1202–1205
White C et al (2006) Improving healthcare quality through distributed diagnosis and home healthcare (D2H2). In: Distributed diagnosis and home healthcare conference, pp 168–172
Wouhaybi R et al (2010) A context-management framework for telemedicine: an emergency medicine case study. Wireless health, San Diego, Oct 2010, pp 164–173
Wu C-C et al (2011) Home self-monitoring of blood flow velocity based on LabVIEW mobile environment. In: IEEE conference on instrumentation and measurement technology, pp 1–3
Zhang Q et al (2010) Research on home health care telemedicine service system concerned with the improvement of medical resources utilization rate and medical conditions. In: International conference on advanced communication technology, pp 1555–1559
Zhang Y, Bai J (2005) performance analysis of a home telemonitoring system. In: IEEE annual conference on engineering in medicine and biology, pp 3950–3953
Zhang Y et al (2009) Agent-based web healthcare systems for real-time chronic disease. In: Proceedings of word conference on services, pp 14–21
Ziefle M, Rocker C, Holzinger A (2011) Medical technology in smart homes: exploring the user’s perspective on privacy, intimacy and trust. In: IEEE annual computer software and applications conference, pp 410–415
ZigBee alliance (2012) http://www.zigbee.org. Accessed 13 Jan 2012
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, K.F. Smart home technology for telemedicine and emergency management. J Ambient Intell Human Comput 4, 535–546 (2013). https://doi.org/10.1007/s12652-012-0129-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12652-012-0129-8