
Abstract
Background
Cost-effectiveness analyses of interventions for older adults have traditionally focused on health status. However, there is increasing recognition of the need to develop new instruments to capture quality of life in a broader sense in the face of age-associated increasing frailty and declining health status, particularly in the economic evaluation of aged and social care interventions that may have positive benefits beyond health.
Objective
To explore the relative importance of health and broader quality of life domains for defining quality of life from the perspective of older South Australians.
Methods
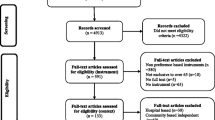
Older adults (n = 21) from a day rehabilitation facility in Southern Adelaide, South Australia attended one of two audio-recorded focus groups. A mixed methods (qualitative and quantitative) study design was adopted. The study included three main components. First was a general group discussion on quality of life and the factors of importance in defining quality of life. Second was a structured ranking exercise in which individuals were asked to rank domains from the brief Older People’s Quality of Life (OPQOL-brief) questionnaire and Adult Social Care Outcomes Toolkit (ASCOT) in order of importance. Third, participants were asked to self-complete the EuroQol five-dimension (EQ-5D), a measure of health status, and two broader quality-of-life measures: the OPQOL-brief and ASCOT.
Results
Mean scores on the EQ-5D, OPQOL-brief and ASCOT were 0.71 (standard deviation [SD] 0.20, range 0.06–1.00), 54.6 (SD 5.5, range 38–61) and 0.87 (SD 0.13, range 0.59–1.00), respectively, with higher scores reflecting better ratings. EQ-5D scores were positively associated with OPQOL-brief (Spearman’s Rho: 0.730; p < 0.01), but not ASCOT. Approximately half (52.4 %) of the participants ranked either ‘health’ or ‘psychological and emotional well-being’ as the domain most important to their quality of life. However, one-third (33.3 %) of the total sample ranked a non-health domain from the ASCOT or OPQOL-brief (safety, dignity, independence) as the most important contributing factor to their overall quality of life. Qualitative analysis of focus group transcripts supported the high value of both health-related (health, psychological well-being) and social (independence, safety) domains to quality of life.
Conclusions
Older adults value both health and social domains as important to their overall quality of life. Future economic evaluations of health, community and aged-care services for older adults should include assessment of both health-related and broader aspects of quality of life.
Similar content being viewed by others


References
Ratcliffe J, Laver K, Couzner L, et al. Health economics and geriatrics: challenges and opportunities. In: Atwood CS, editor. Geriatrics: InTech. http://www.intechopen.com/articles/show/title/health-economic-evaluation-and-geriatrics-challenges-and-opportunities; 2012.
Australian Government Productivity Commission. Economic implications of an ageing Australia. Canberra; 2005.
National Health and Hospitals Reform Commission. A Healthier Future for all Australians. Canberra; 2009.
Brazier J, Ratcliffe J, Salomon J, et al. Measuring and valuing health benefits for economic evaluation. Oxford: Oxford University Press; 2007.
Drummond M, Sculpher M, Torrance G, et al. Methods for the economic evaluation of health care programmes. 3rd ed. New York: Oxford University Press; 2005.
Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33:337–43.
Crotty M, Ratcliffe J. If Mohammed won’t come to the mountain, the mountain must go to Mohammed. Age Ageing. 2011;40:290–2.
Stott DJ, Langhorne P, Knight PV. Multidisciplinary care for elderly people in the community. Lancet. 2008;371:699–700.
Osborne RH, Hawthorne G, Lew EA, et al. Quality of life assessment in the community-dwelling elderly: validation of the Assessment of Quality of Life (AQoL) Instrument and comparison with the SF-36. J Clin Epidemiol. 2003;56:138–47.
Ratcliffe J, Laver K, Couzner L, et al. Not just about costs: the role of health economics in facilitating decision making in aged care. Age Ageing. 2010;39:426–9.
Coast J, Flynn TN, Natarajan L, et al. Valuing the ICECAP capability index for older people. Soc Sci Med. 2008;67:874–82.
Netten A, Burge P, Malley J, et al. Outcomes of social care for adults: developing a preference-weighted measure. Health Technol Assess. 2012;16:1–166.
Bowling A, Stenner P. Which measure of quality of life performs best in older age? A comparison of the OPQOL, CASP-19 and WHOQOL-OLD. J Epidemiol Community Health. 2011;65:273–80.
Bowling A. The psychometric properties of the older people’s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Curr Gerontol Geriatr Res. 2009; ID 298950.
Bowling A, Hankins M, Windle G, et al. A short measure of quality of life in older age: The performance of the brief Older People’s Quality of Life questionnaire (OPQOL-brief). Arch Gerontol Geriatr. 2013;56:181–7.
Brod M, Tesler LE, Christensen TL. Qualitative research and content validity: developing best practices based on science and experience. Qual Life Res. 2009;18:1263–78.
Davis JC, Liu-Ambrose T, Richardson CG, et al. A comparison of the ICECAP-O with EQ-5D in a falls prevention clinical setting: are they complements or substitutes? Qual Life Res. 2013;22:969–77.
Couzner L, Ratcliffe J, Crotty M. The relationship between quality of life, health and care transition: an empirical comparison in an older post-acute population. Health Qual Life Outcomes. 2012;10:69.
Bowling A, Gabriel Z, Dykes J, et al. Let’s ask them: a national survey of definitions of quality of life and its enhancement among people aged 65 and over. Int J Aging Hum Dev. 2003;56:269–306.
Fry PS. Whose quality of life is it anyway? Why not ask seniors to tell us about it? Int J Aging Hum Dev. 2000;50:361–83.
Bowling A, Iliffe S. Which model of successful ageing should be used? Baseline findings from a British longitudinal survey of ageing. Age Ageing. 2006;35:607–14.
Bowling A. Aspirations for older age in the 21st century: what is successful aging? Int J Aging Hum Dev. 2007;64:263–97.
Bilotta C, Bowling A, Nicolini P, et al. Older People’s Quality of Life (OPQOL) scores and adverse health outcomes at a one-year follow-up. A prospective cohort study on older outpatients living in the community in Italy. Health Qual Life Outcomes. 2011;9:72.
Malley JN, Towers AM, Netten AP, et al. An assessment of the construct validity of the ASCOT measure of social care-related quality of life with older people. Health Qual Life Outcomes. 2012;10:21.
Acknowledgments
There are no sources of funding to disclose for this manuscript. The authors declare no conflicts of interest. CM, JR and RW initiated the study and contributed to data collection and analysis. All authors contributed to interpretation of results. CM drafted the manuscript. All authors read, edited and approved the final manuscript. JR is the guarantor for the overall content. Thank you to the staff and patients of the Repatriation General Hospital who participated in this study. We gratefully acknowledge Professor Maria Crotty for facilitating the recruitment of volunteers.
Author information
Authors and Affiliations
Corresponding author
Appendix: Standardised Script and Instructions from Focus Groups
Appendix: Standardised Script and Instructions from Focus Groups
Introduction and consent
TASK 1. Collect health status (EQ-5D)
TASK 2. Focus group
“Let’s start by talking about quality of life generally. Tell me about what quality of life means to you.”
Prompts
-
Examples of dimensions to quality of life
“We’ve been talking about different items which contribute to quality of life and now I’d like to move on to talk about which factors are most important to you.”
Distribute cards containing quality of life dimensions for OPQOL OR ASCOT (i.e. health, social relationships, independence, personal control etc.):
“We would like you to rank the items on these cards in order of importance (most to least important) on your own.”
Prompts
-
The researchers will describe what they mean by ranking with an example.
-
Why did you rank this item as most/least important?
Record order life dimensions are placed in by each volunteer.
Repeat for other measure (i.e. OPQOL or ASCOT)
Distribute new set of cards containing life dimensions from both ASCOT and OPQOL.
“We would like you to pick out your top 4 items you think are most important to your quality of life.”
Record top four for each person. All group members will be invited to share their selection and why.
“Do you think any of these items are not important and should not be included when we talk about quality of life?”
Prompts
-
The researchers will describe what they mean by excluding items.
-
Why do you think this should not be included?
“Do you think there is anything that is important to your quality of life which is missing from the cards we have given you and you think should be included?”
Prompts
-
Give examples.
-
Why do you think this is important?
“So, we’ve talked about what is important to you in your life. In this last part we would like you to complete two questionnaires about quality of life. You will come across items familiar to you from the previous ranking exercises.”
TASK 3. Distribute the ASCOT and OPQoL for completion by participants. After completed:
“What do you think about these questionnaires?”
Prompts
-
Were the questionnaires easy to complete?
-
Did they cover all aspects of life you think are important?
“Is there anything you would like to add?”
Rights and permissions
About this article
Cite this article
Milte, C.M., Walker, R., Luszcz, M.A. et al. How Important Is Health Status in Defining Quality of Life for Older People? An Exploratory Study of the Views of Older South Australians. Appl Health Econ Health Policy 12, 73–84 (2014). https://doi.org/10.1007/s40258-013-0068-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-013-0068-3