
Abstract
The QT interval on the electrocardiogram is the time from the onset of ventricular depolarisation (the Q wave) to completion of repolarisation (the end of the T wave). It is influenced by heart rate, autonomic factors, electrolyte levels, gender and age. A prolonged QT interval indicates an increased risk of developing malignant ventricular tachyarrhythmias, particularly torsade de pointes. QT prolongation may be primary (inherited, familial, congenital, idiopathic) or caused by disease, drugs or toxins.
Drugs that have been associated with the development of torsade de pointes include antiarrhythmic, antibacterial and psychotropic agents and antihistamines. Several of these drugs depress myocardial ion channels, particularly the rapidly activating delayed rectifier (repolarising) potassium current (IKr). Overdosage of drugs that affect the delayed rectifier (repolarising) potassium currents (Ik), or coadministration of these drugs with another medication that inhibits their metabolism (e.g. an antihistamine such as terfenadine with an antifungal agent such as ketoconazole, which inhibits the cytochrome P450 3A4 hepatic enzyme), can induce torsade de pointes.
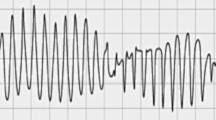
Torsade de pointes is a potentially life-threatening ventricular tachyarrhythmia and the risks of administering drugs that can induce this condition must be carefully considered.
Similar content being viewed by others


References
Sagie A, Larson MG, Goldeberg RJ, et al. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol 1992; 70: 797–801
Bazett HC. An analysis of time relations of electrocardiograms. Heart 1920; 7: 353–67
Fridericia LS. Die systolendauer in elektrokardiogramm bei normalen menschen and bei herzkranken. Acta Med Scand 1920; 53: 469–86
Shipley RA, Hallaran WR. Four-lead electrocardiogram in 200 normal men and women. Am Heart J 1936; 11: 325–45
Goldman MJ. Principles of clinical electrocardiography. 8th ed. Los Altos, CA: Lange Medical Publications, 1973: 24–8
Lepeschkin E. Modern electrocardiography. Vol. 1. Baltimore: William & Wilkins, 1951
Moss AJ. Measurement of the QT interval and the risk associated with QTc interval prolongation: a review. Am J Cardiol 1993; 72: 21–3B
Moss AJ, Robinson JL. The long-QT syndrome: genetic considerations. Trends Cardiovasc Med 1992; 2: 81–3
Roden DM, Lazzara R, Rosen M, et al. for the SADS Foundation Task Force on LQTS. Multiple mechanisms in the long-QT syndrome: current knowledge, gaps, and future directions. Circulation 1996; 94: 1996–2012
Wang Q, Curran ME, Splawski I, et al. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet 1996; 12: 17–23
Sanguinetti MC, Curran ME, Zou A, et al. Coassembly of KvLQTl and minK (IsK) proteins to form cardiac IKs potassium channel. Nature 1996; 384: 80–83
Curran ME, Splawski I, Timothy K, et al. A molecular basis for cardiac arrhythmia: HERG mutations cause long QT syndrome. Cell 1995; 80: 795–803
McDonald TV, Yu Z, Ming Z, et al. A minK-HERG complex regulates the cardiac potassium current IK1. Nature 1997; 388: 289–92
Wang Q, Shen J, Splawski I, et al. SCN5A mutations cause an inherited cardiac arrhythmia, long QT syndrome. Cell 1995; 80:805–11
Sicouri S, Antzelevitch C. A subpopulation of cells with unique electrophysiological properties in the deep subepicardium of the canine ventricle: the M cell. Circ Res 1991; 68: 1729–41
Dessertenne F. La tachycardic ventriculaire a deux foyers opposes variables. Arch Mal Coeur 1966; 59: 263–72
Honig PK, Wortham DC, Zamani K, et al. Terfenadine-keto-conazole interaction: pharmacokinetic and electrocardio-graphic consequences. JAMA 1993; 269: 1513–8
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Moss, A.J. The QT Interval and Torsade de Pointes. Drug-Safety 21 (Suppl 1), 5–10 (1999). https://doi.org/10.2165/00002018-199921001-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-199921001-00002