1. Introduction
Robotic surgery is the paragon of the amalgamation of engineering and surgical skill. Until fairly recently, robot-assisted surgery was a phantom of the mind, but after the first abdominal procedure in 1997 by a Belgian surgeon, Jaques Himpens, the field of robot-assisted abdominal surgery has greatly expanded [
1]. Within a decade, robot-assisted surgery has been piloted for procedures spanning from the undemanding to the highly complex [
2]. Despite considerable acquisition and maintenance costs, robotic systems are available in tertiary centers worldwide [
3].
Robotic surgery offers certain benefits to the surgeon, including protective ergonomics for musculoskeletal health and the decrease of cognitive fatigue, but evidence on the benefits to the patient is less apparent [
4]. Due to increased degrees of freedom and tremor elimination, robot-assisted surgery is speculated to lead to lower conversion rates as complex movements can be performed within a confined space. Emphasized advantages of liver robot-assisted surgery include the lower risk of postoperative ascites, infection and pain [
3]. Some authors speculate that robot-assisted hepatectomy is particularly beneficial for HCC patients with cirrhosis [
5].
With exception of rare genetic cases, HCCs develop in the background of liver disease. Whether due to viral hepatitis, metabolic dysfunction-associated, or alcohol-related liver disease, hepatic parenchyma undergoes structural changes that may range from inflammation, steatosis, fibrosis, to cirrhosis. Although a sequential progression to cirrhosis is not a prerequisite, most non-tumor tissue in HCC patients has some degree of damage. A global problem on the rise is a metabolic dysfunction-associated liver disease (MAFLD), which is associated with an increased risk of post-hepatectomy liver failure (PHLF) in patients undergoing liver resection [
6]. Cirrhosis is already an established factor for PHLF [
7]. With the continued rise of liver disease and the high prevalence of liver cancer, the importance of strategies for curative treatment are rising as well. Surgeons must balance the risk of PHLF and the benefit of hepatectomy while evaluating patients suitable for surgery. Expanding the techniques available and offering the safest treatment options, even at potentially higher material and maintenance costs, is a priority in hepatobiliary surgery. The aim of this systematic review and meta-analysis was to compare the outcomes of robot-assisted hepatectomy (RAH) to open (OH) and laparoscopic (LH) approaches in HCC patients based on current available studies.
2. Materials and Methods
The systematic review and meta-analysis has been conceptualized and is reported in accordance with current PRISMA guidelines [
8], as well as in the recommendations of the Cochrane Handbook for Systematic Reviews and Interventions [
9]. The protocol has been registered on the PROSPERO international prospective register prior to data extraction (PROSPERO 2022 CRD42022328544). The following PICOS criteria were defined:
Population: patients undergoing hepatectomy for HCC
Intervention: Robot-assisted hepatectomy
Comparison: Laparoscopic or open hepatectomy
Outcomes: complications (overall, major, minor), PHLF, ascites, biliary leak, hemorrhage, infections, conversion rates, recurrence, overall survival, and recurrence free survival.
Recent recommendations were used for the structured literature search [
10]. MEDLINE via PubMed, Web of Science and Cochrane Library were searched for publications on HCC resection with robotic approaches without restriction on language or publication date (see
Supplementary File S1 for full search strategy). Reference lists of included studies were hand-searched for potentially relevant publications. All publications with comparative study methodology were included, without restriction on prospective or retrospective design, blinding, or randomization. Communications, comments and letters to the editor, editorials, meeting abstracts, and reviews were excluded. Two independent reviewers (AML and JF) performed the title and abstract screening and subsequent full text review. All disagreements were resolved through discussion and consultation with the third reviewer (KH).
Extraction of data from included studies was performed by two independent reviewers (AML and JF). For data extraction, a standardized form composed prior to the study was utilized and adjusted after first two data extractions. The following data was documented for each publication: title, authors, country, year of publication, journal, funding, study design, interventions, demographics, and clinical outcomes (conversion and complication rates, post-hepatectomy liver failure, ascites, biliary leakage, bleeding, infections, Clavien-Dindo, mortality, recurrence, overall and recurrence-free survivals).
Meta-analyses were performed using publicly available RStudio software, version 4.0.3. The “Metafor”, “meta”, “ggplot2”, and “survival” packages were used. A random-effects model was used for effect estimates for all outcomes due to the anticipated heterogeneity in methodology and clinical framework of relevant studies. Statistical heterogeneity was evaluated using the I2 statistics. An I2 value below 25% indicated low, and over 75% indicated high heterogeneity. The Mantel-Haenszel method was used for pooling odds ratios and 95% confidence intervals in dichotomous endpoints. Aggregated data was compared between groups. Categorical values were compared with an χ2 test, while an independent sample t-test was used for continuous variables. Survival was assessed using the Kaplan-Meier method.
The methodological quality of included studies was evaluated with ROBINS-I [
11] and the certainty of evidence was assessed using GRADE [
12] for significant outcomes and outcomes reported by three or more studies.
3. Results
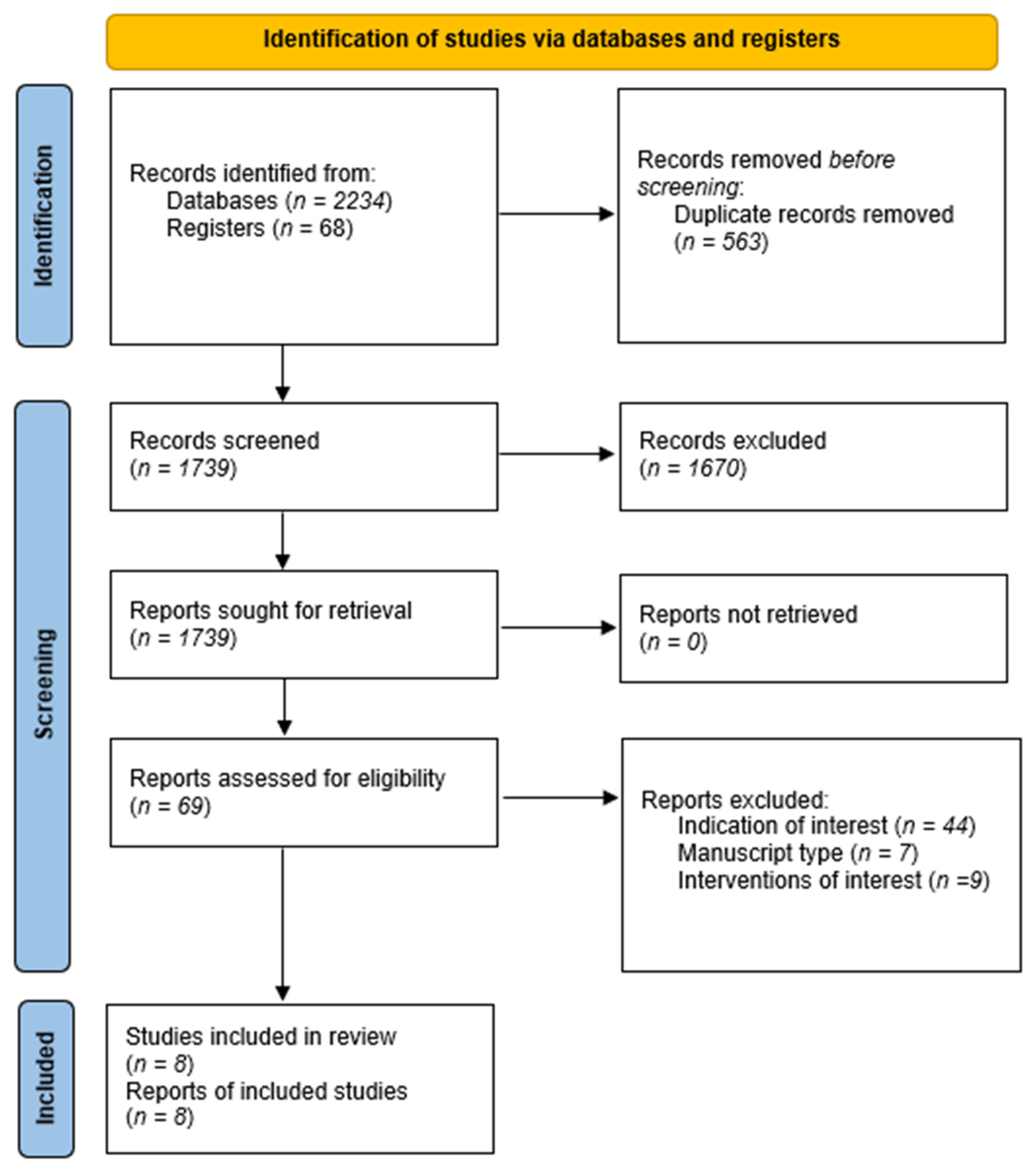
After exclusion of duplicates, 1739 records were screened, from which 69 were assessed for eligibility. After exclusion of articles that did not study the indication or intervention of interest, as well as manuscript types, eight studies were included in the analysis. The overview of the study selection process is depicted in
Figure 1 and a description of included studies is provided in
Table 1.
All studies were of retrospective design; five studies compared RAH to LH [
13,
15,
16,
17,
18]. A comparison between OH and RAH was done by three studies [
14,
19,
20]. There were no randomized controlled trials available and no study focused on cirrhotic patients exclusively.
3.1. Critical Appraisal of Included Studies
The risk of bias was assessed using ROBINS-I and included the assessment of seven domains: bias due to confounding, selection, classification of interventions, missing data, measurement of outcomes, and reported results. Overall, the risk of bias in studies was low (
Table 2).
3.2. Characteristics of Included Studies and Patients in RAH and LH Comparisons
The five studies comparing RAH and LH had retrospective designs, and only one performed a propensity score matching for the two groups. Overall, 529 patients after LH were compared to 324 patients after RAH (
Table 3). The primary identified liver disease in both studies was viral, and the distribution of background liver disease was similar between groups.
Concerning tumor characteristics, only differentiation could be assessed between groups, as no other characteristic was provided by multiple studies. The differentiation of HCC was similar between groups, with G1 in 85 vs. 36, G2 155 vs. 68, and G3/G4 36 vs. 23 cases, in LH and RAH, respectively.
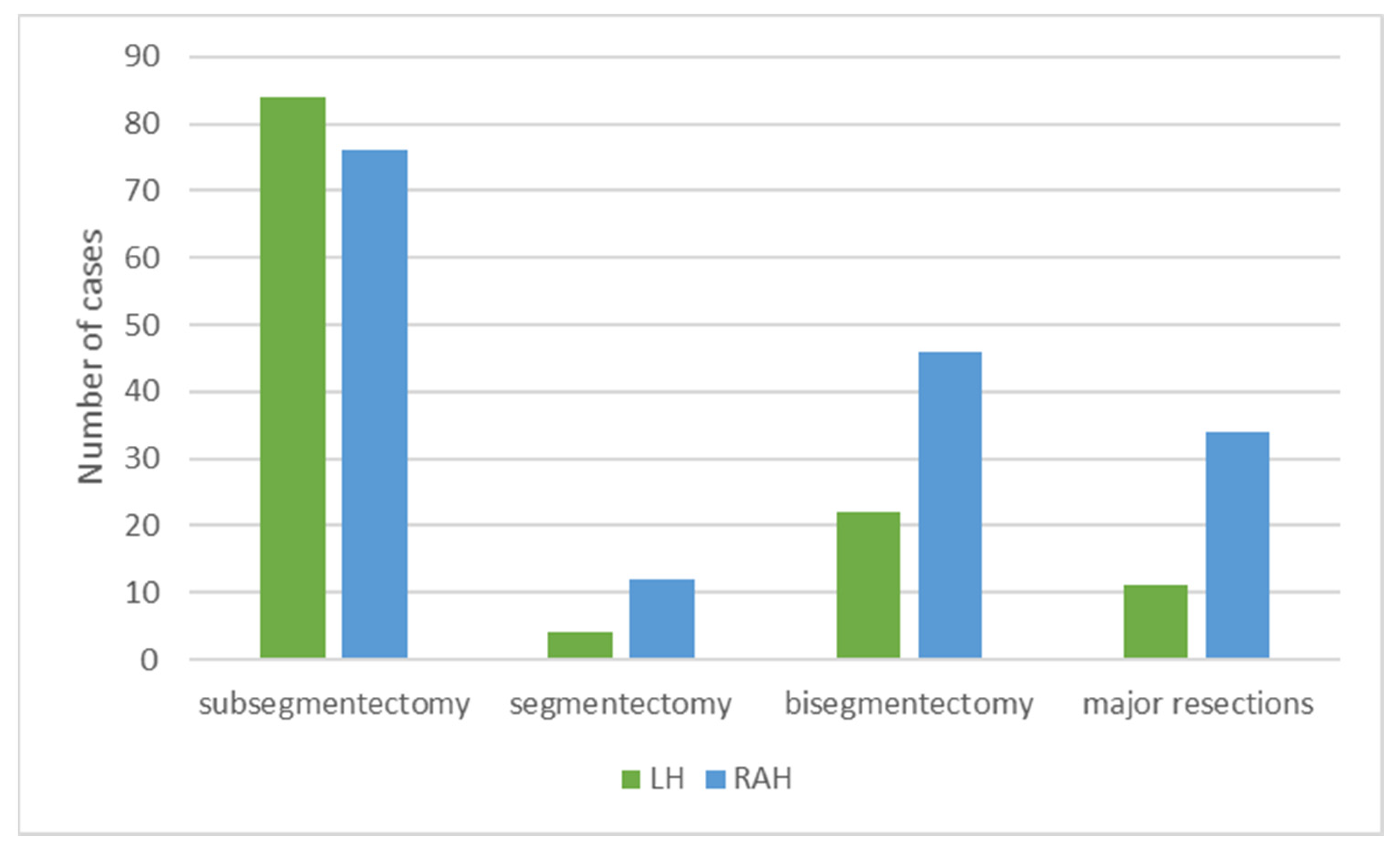
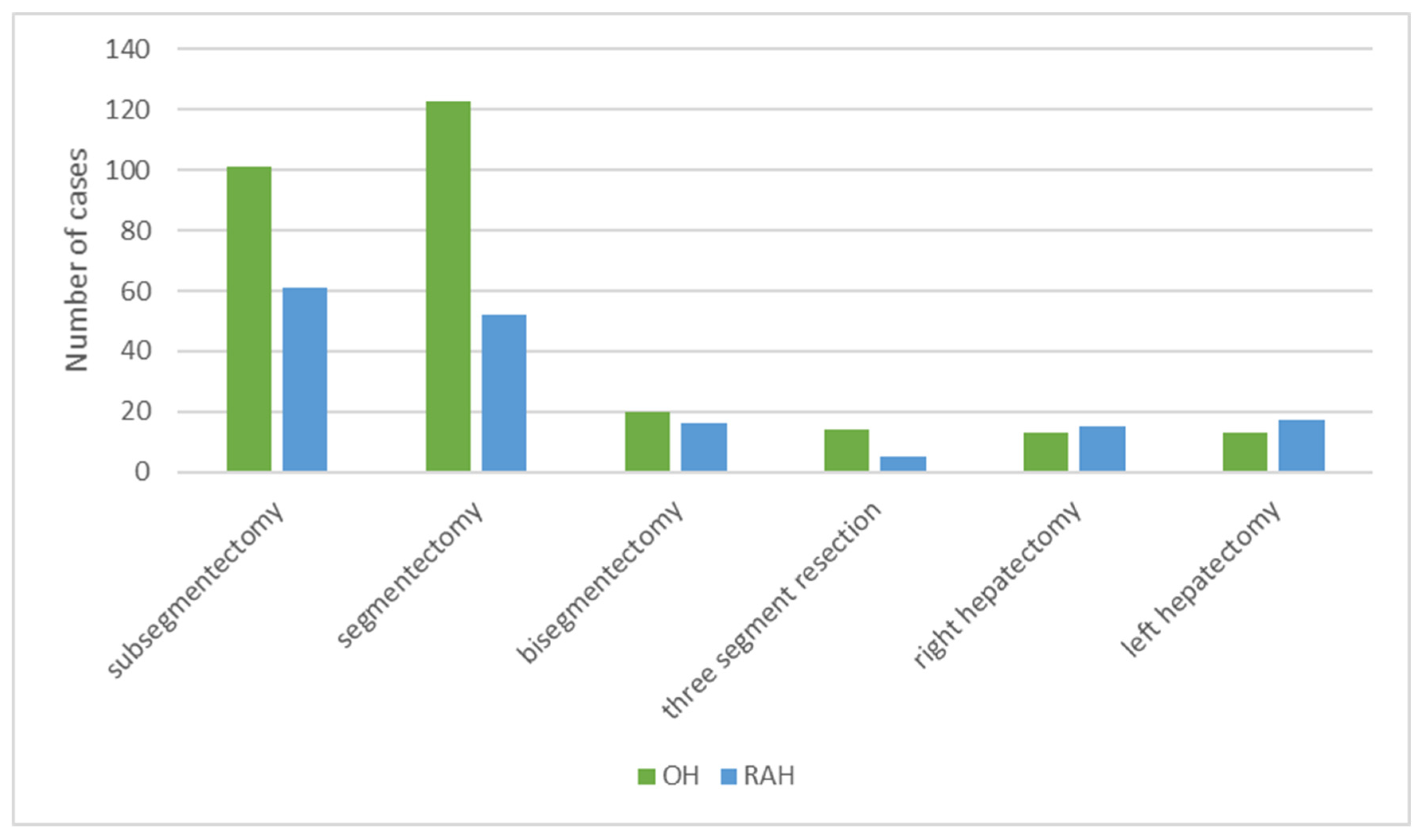
The distribution of surgeries performed was significantly different [χ
2 = (1, 368) = 7.5583,
p = 0.006], as more major resections were performed in the RAH than LH. However, the pooled comparison was based on four studies, while the largest study omitted the data (
Figure 2).
3.3. Comparison between RAH and LH
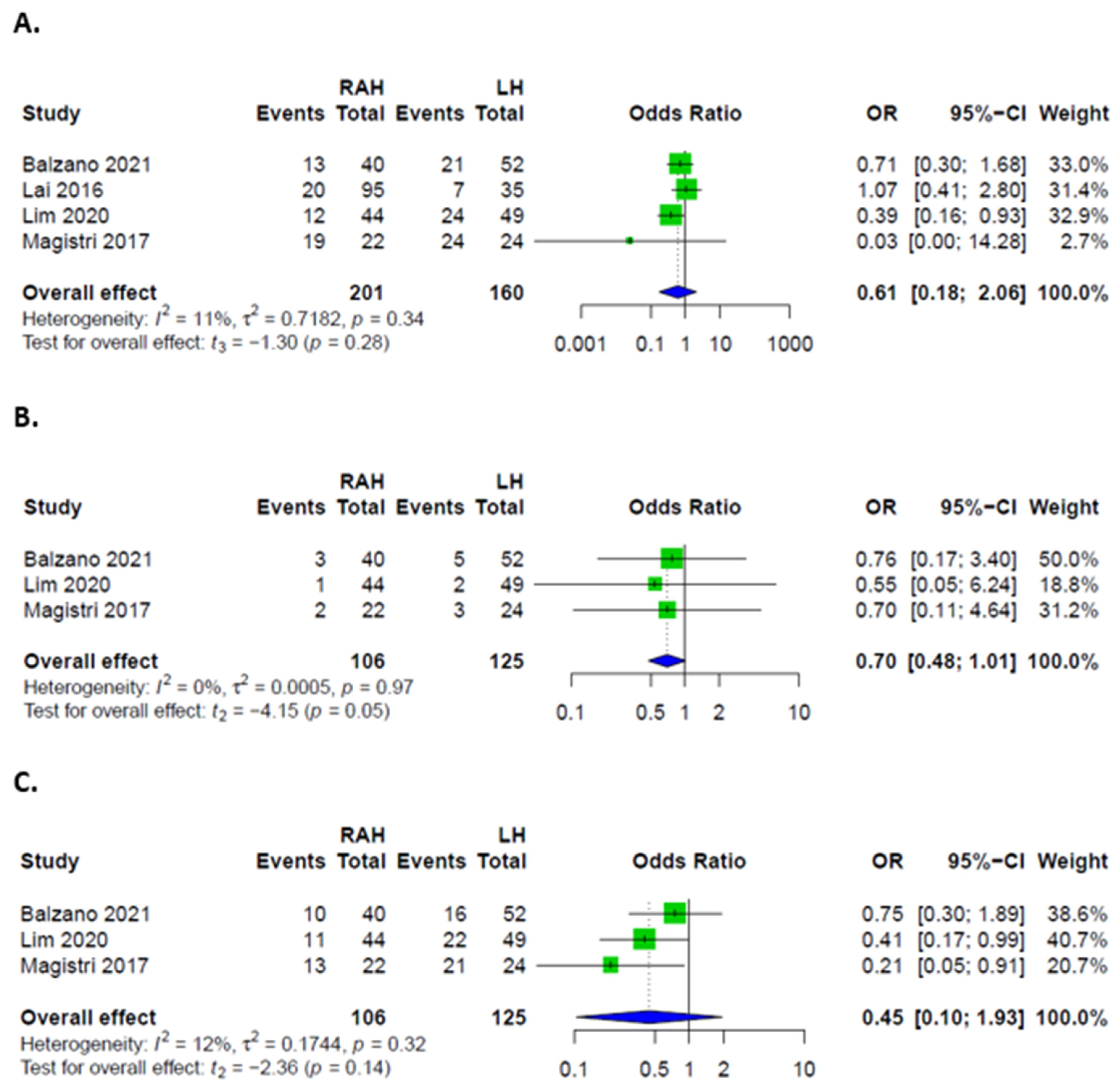
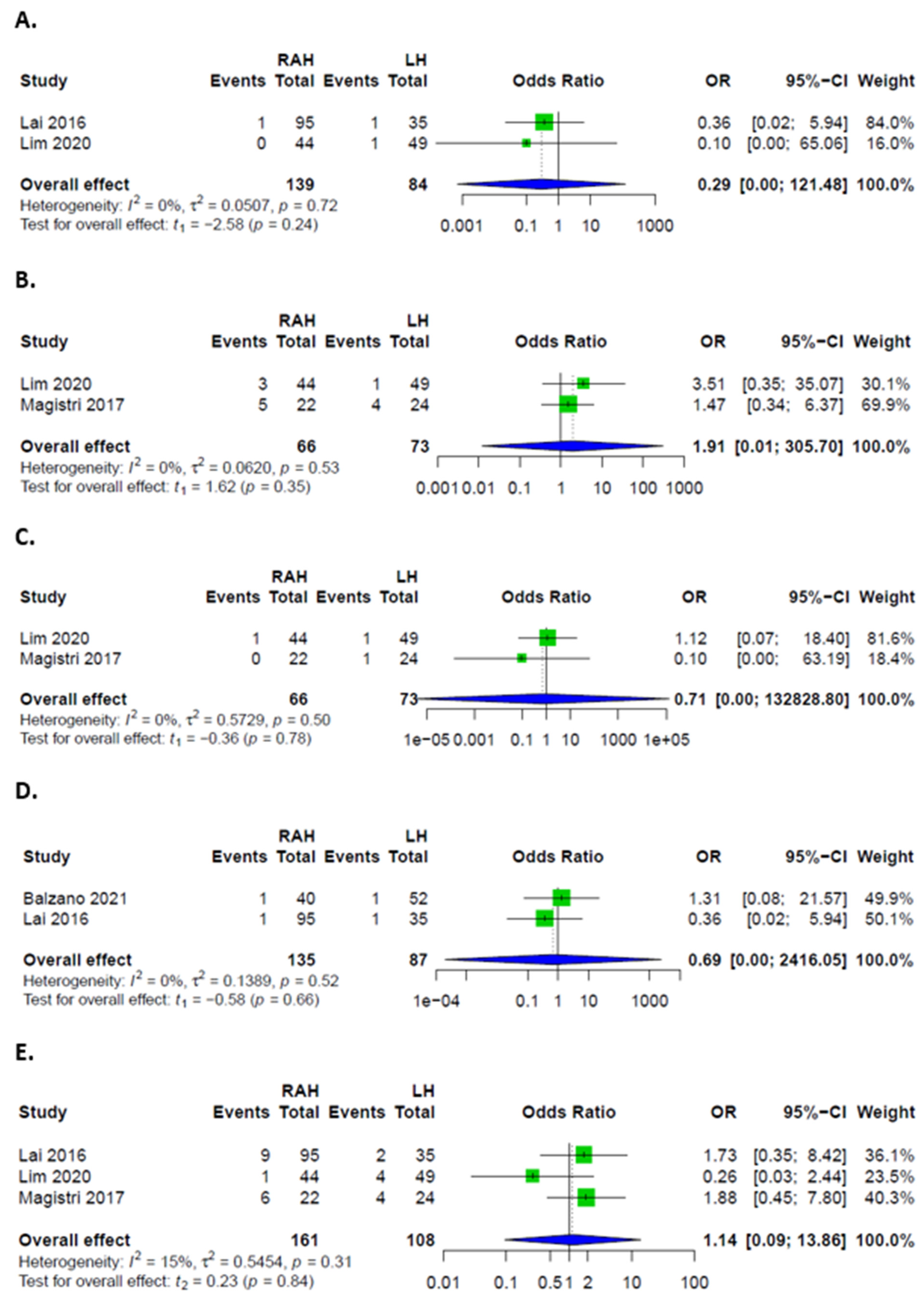
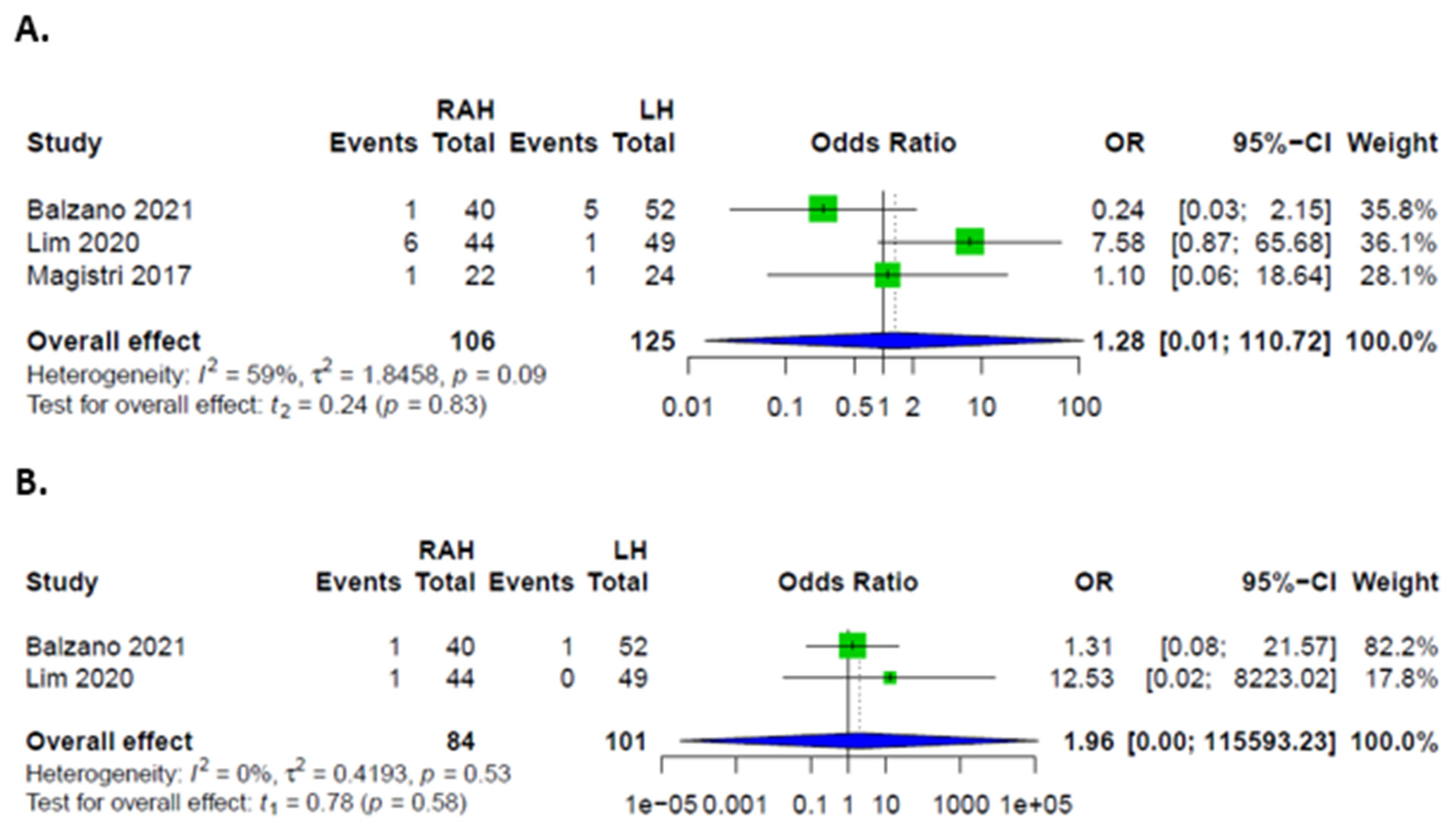
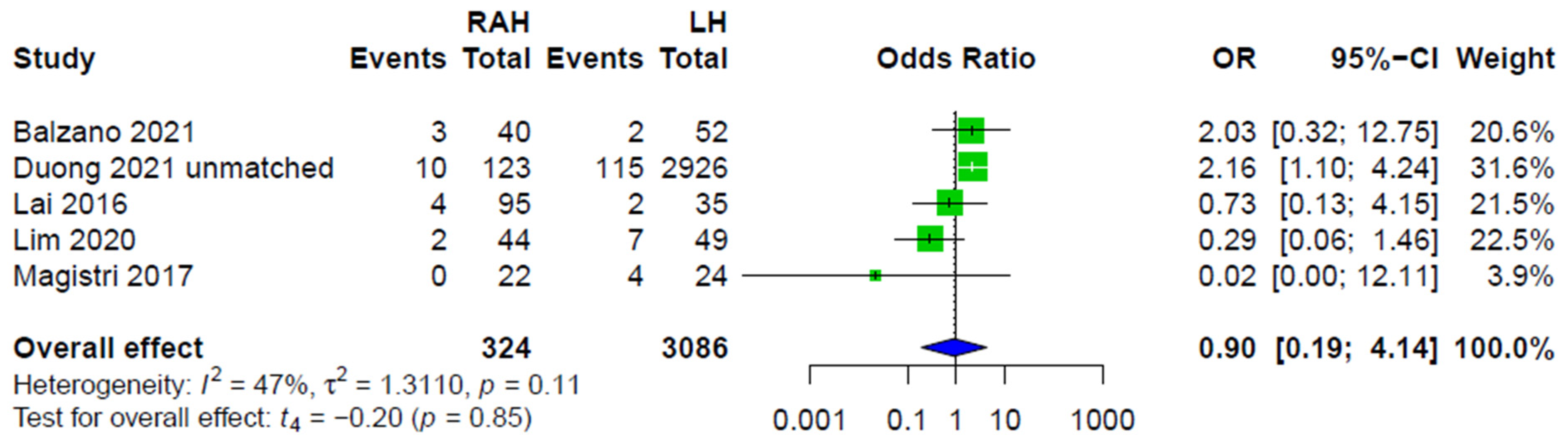
Overall, there were no significant differences in complication rates between RAH and LH. Rates of major complications, defined as Clavien-Dindo grades III and IV, were higher in LH. Patients had similar odds of developing minor complications, as well as PHLF, ascites, biliary leakages, hemorrhages, and infections in both groups (
Figure 3 and
Figure 4). Rates of intraoperative transfusions and reoperations were similar as well (
Figure 5). No mortality was described for either group in the included studies.
All five studies comparing LH to RAH provided data on conversion, and summary effect did not show significant differences between the LH and RAH approaches (
Figure 6).
No data was provided to evaluate functional recovery, e.g., mobilization or physical activity levels. Studies did not provide data to evaluate ICU/IMC length of stay.
3.4. Oncological Outcome in Patients after RAH and LH Approaches
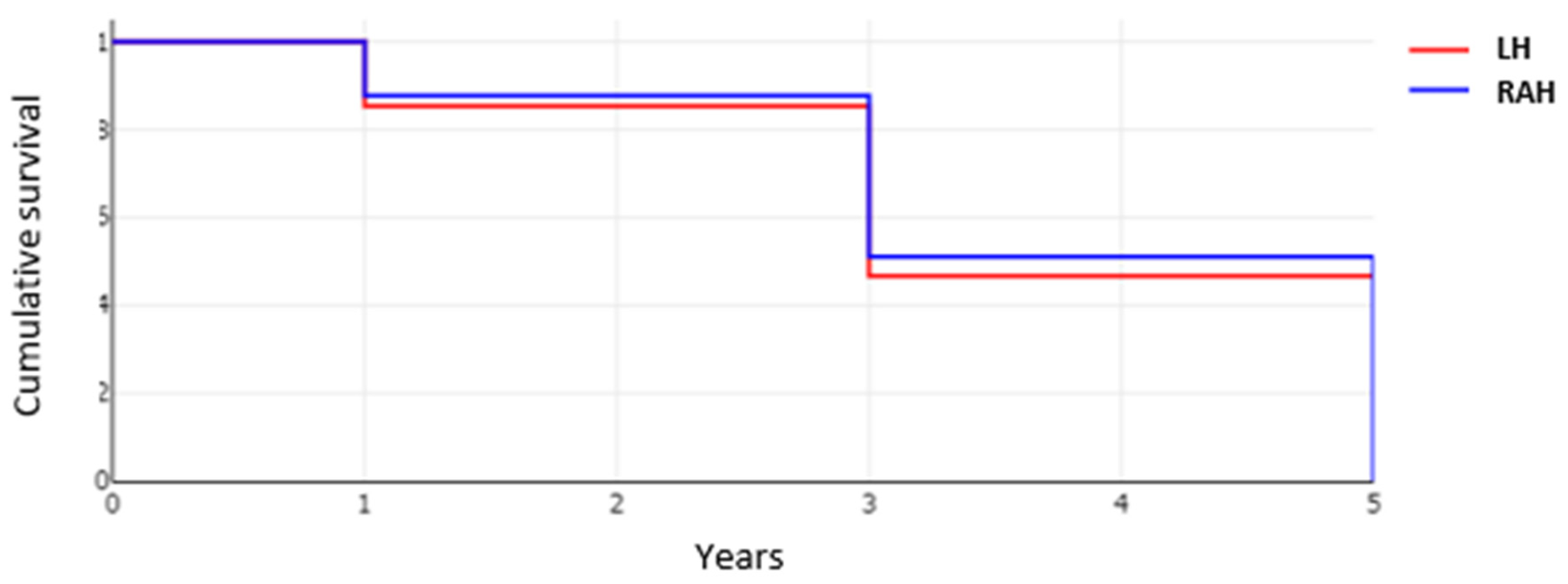
Clear resection margin (R0) was significantly more often achieved in the RAH group with 96.8% (152 of 157 cases), than in the LH group, with 91.0% (101 of 111 cases) (
p = 0.041). Recurrence rates were similar in both groups with 35.6% of patients (48 of 135) in the RAH and 46.0% cases (40 of 87) developing a recurrence within up to five years of follow-up (
p = 0.12). The overall survival after surgery was comparable between the two groups (
p = 0.769) (
Figure 7).
3.5. Characteristics of Included Studies and Patients in RAH and OH Comparisons
Three retrospective studies, one of them PSM, compared the OH and RAH approaches. An RAH group of 167 was compared against 289 patients in the OH group. Pooled data on patient demographics is provided in
Table 4. In total, 244 minor and 45 major surgeries were performed openly and 129 minor and 38 major hepatectomies were robot-assisted (
p = 0.06) (
Figure 8).
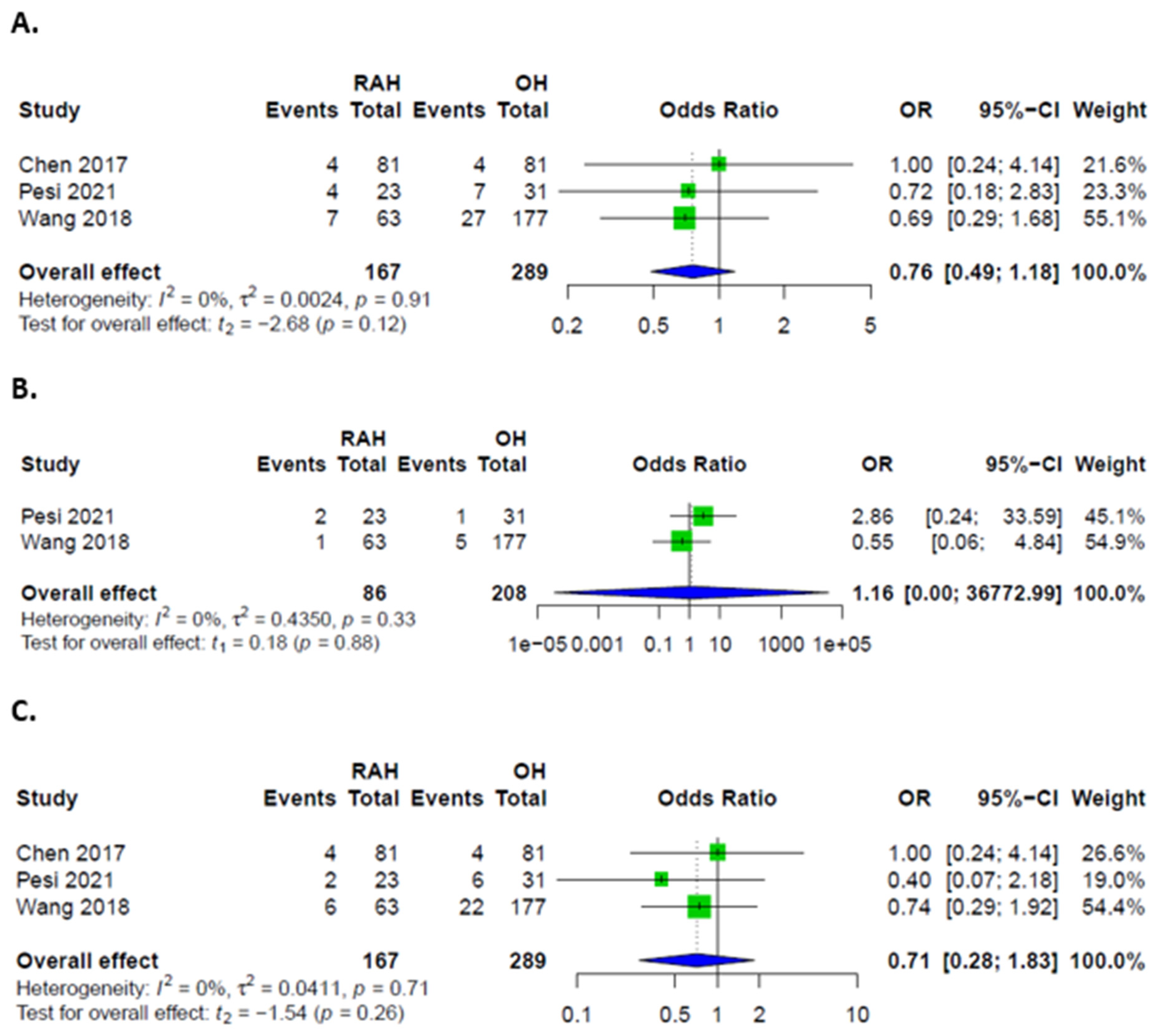
3.6. Comparison between RAH and OH
Overall, major and minor complications were comparable between the two groups (
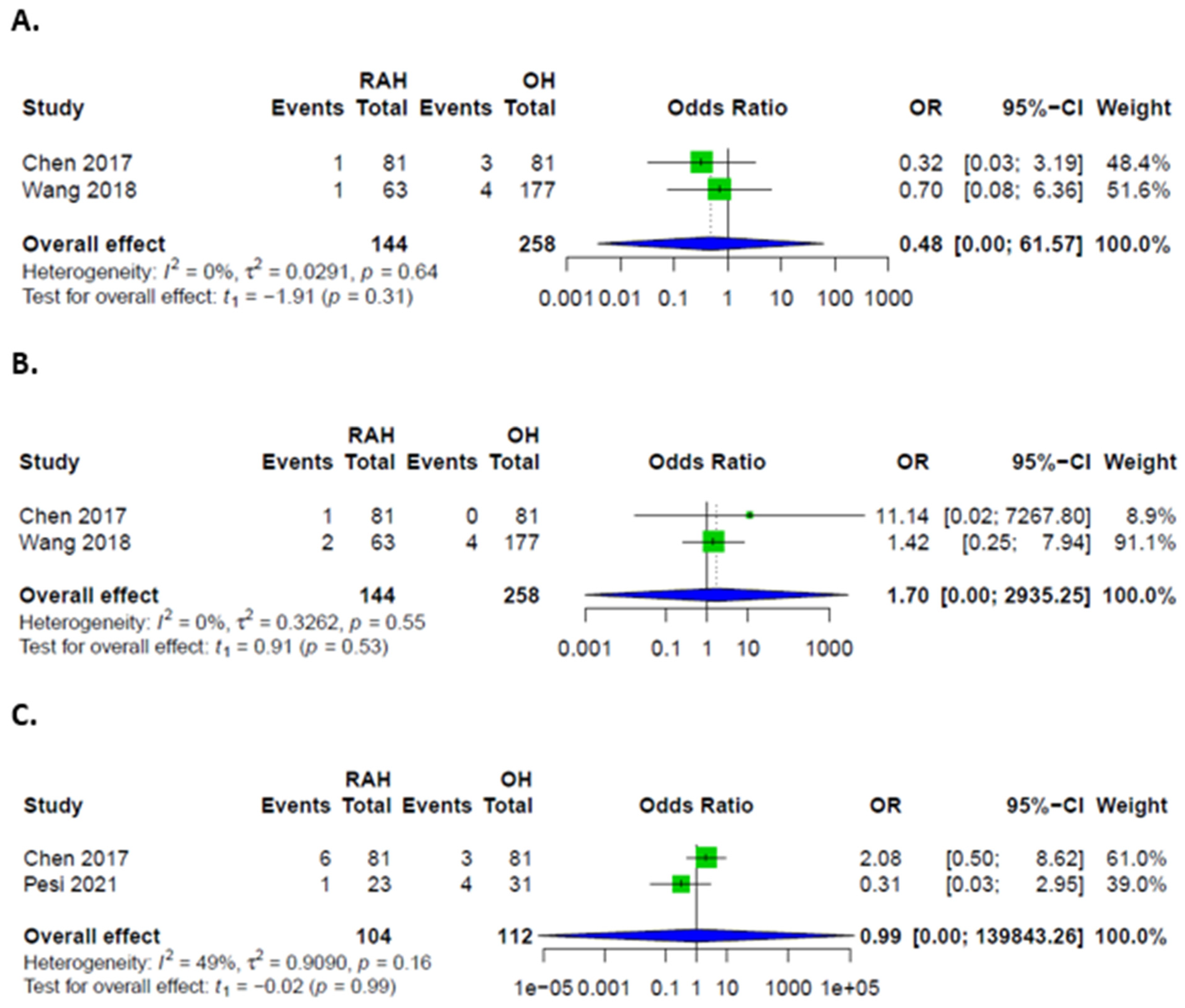
Figure 9). Specific complications could only be assessed for biliary leakages and hemorrhages, which were also comparable (
Figure 10). PHLF was only described in one case, which was resected via the open approach. Ascites was additionally described by one study in 10 cases in the OH and one case in the RAH group. Concerning additional interventions, only sufficient data on transfusions was provided, without significant difference between groups (
Figure 10). No data was provided to evaluate functional recovery, e.g., mobilization or physical activity levels. Total hospital stay, as well as ICU/IMC length of stay, could not be pooled for analysis.
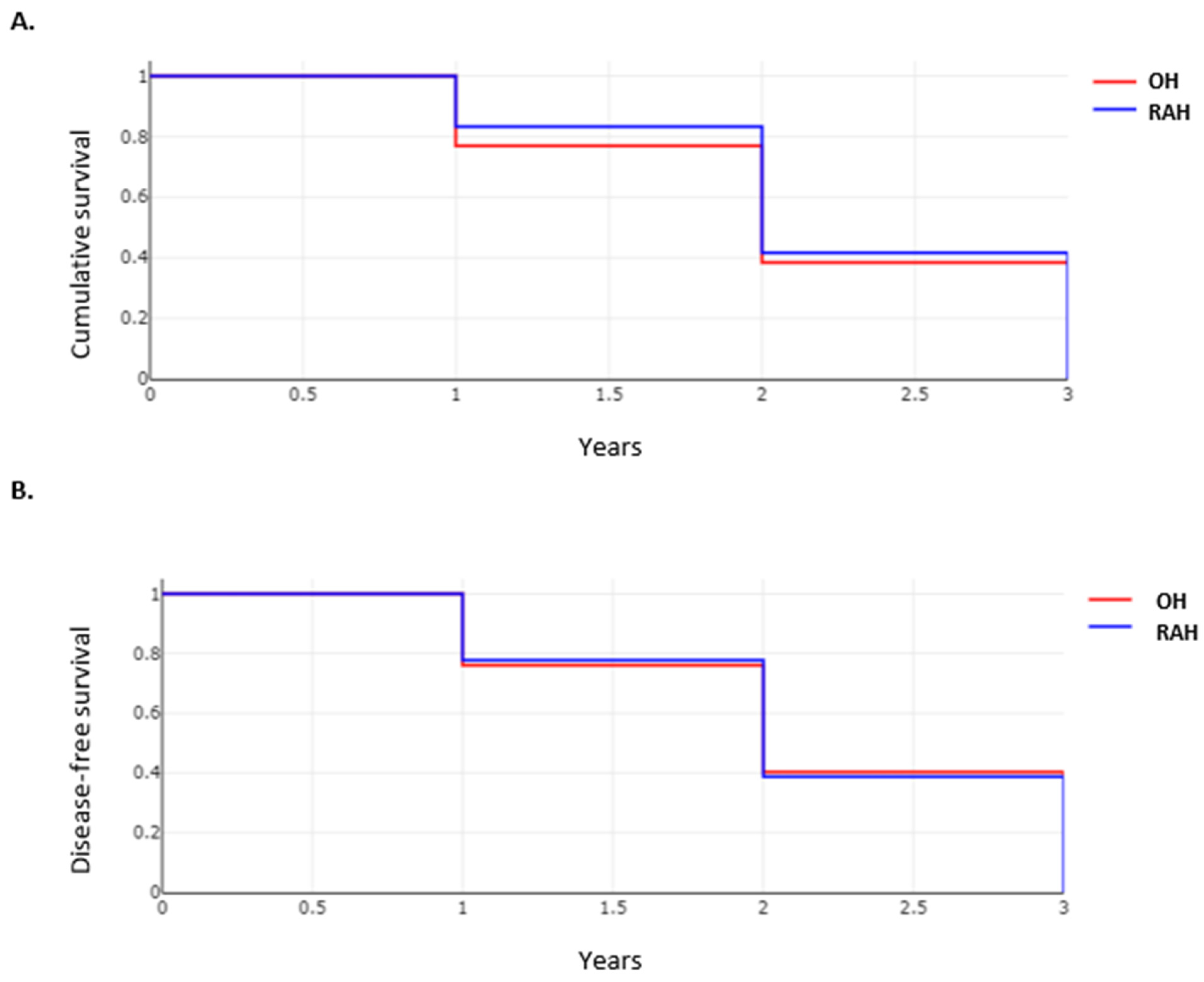
3.7. Oncological Outcome in Patients after RAH and OH Approaches
Resection margins were comparable between the two groups, with R0 achieved in 97.2% of cases (281 of 289) in the OH group vs. 96.4% cases (161 of 167) in the RAH group (
p = 0.6). Recurrence rates were only reported in one study, but overall and disease-free survivals were aggregated from two studies and are depicted in
Figure 11. No difference was observed in overall and disease-free survivals between the two groups.
3.8. Certainty of Evidence
A Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was utilized to rate the certainty of evidence. The main outcomes are listed in
Table 5. Overall, due to the exclusively retrospective study design and lack of matching in most included studies, the certainty of evidence ranged from low to very low.
4. Discussion
Robot-assisted surgery has gained popularity among surgeons and developers, and it is an approach that will change the future of abdominal surgery [
3]. The allure is not merely that of novelty but of possibilities. It has the potential to provide access to minimally invasive surgery specialists where the distance would otherwise preclude it [
21]. Additionally, due to elegant engineering, robot-assisted surgery is able to offer precision surgery while eliminating imprecision due to hand tremors [
22]. Despite potentialities that the surgeons expect, robot-assisted surgery needs meticulous elucidation. Although benefits are suggested in certain patient groups, like cirrhotic patients undergoing liver resection, the evidence to support this claim is clearly lacking [
5]. Thus far, studies have not been focused on patients with cirrhosis. Not only did the studies not differ statistically in number of cirrhotic patients undergoing RAH or another approach, it was mostly unclear how cirrhotic patients were identified and defined. Furthermore, there are no randomized controlled trials comparing RAH, LH and open surgery. Additionally, no studies compared material costs in addition to cost and revenue within the reimbursement system.
With MAFLD rising as the cause of HCC and NAFLD being associated with higher PHLF rates, an interesting question to examine is the influence of steatosis, fibrosis and NASH on outcomes in RAH versus LH or OH. This is particularly relevant, as obesity, frequently concurring in MAFLD patients, may pose an additional limitation for minimally invasive surgery, and the benefits of the RAH approach would be interesting to consider [
6].
Although RAH offers some benefits that may potentially lead to lower complication rates, such as enabling elaborate motions in limited space, the current evidence suggests that, so far, RAH is only comparable to LH or OH. In particular, few liver specific complications are reported for either approach, which may indicate that on one hand, hepatectomy has become a fairly safe procedure at hospitals offering state-of-the-art techniques, but also that a wider patient selection is needed to evaluate the approaches. Although functional recovery is often the primary reason for minimally invasive surgery and, more recently, robot-assisted surgery, mobilization, return to physical activity, pain levels, and quality of life has not been reported by studies thus far. Total length of hospital stay is similar for RAH and LH, but whether ICU/IMC observation is comparable as well remains unclear. The lengths of stay are underreported in comparisons between RAH and OH. Our study is the first systematic review to specifically investigate the impact of RAH versus LH or OH in patients with HCC. According to our results, RAH achieves comparable outcomes as LH and OH. Suggested significant benefits for cirrhotic patients were not confirmed by the present meta-analysis due to lack of well-designed clinical trials and real evidence.
A limitation for the certainty of evidence is the designs of the included studies, as they were all retrospective in nature, with only two studies attempting to match patient groups through propensity-scores [
14,
18]. Although retrospective evidence suggests that RAH is a robust approach in patients with HCC, prospective studies, in particular RCTs, are needed to truly evaluate whether RAH offers benefits. The largest included retrospective study has omitted the data on procedure distribution, which in turn poses a bias in the comparison of complications [
15]. As one of the arguments for RAH is the gentler approach that may reduce liver-specific complications, RCTs will need to be sufficiently powered to evaluate the occurrence of PHLF in patients treated with various approaches. As studies reported so far only included one case of PHLF in patients after RAH versus two in patients after LH, clinicians contemplating an RCTs will need to consider the numbers to treat accordingly. Homogeneity also needs to be considered, and the pooling of major and minor hepatectomies into one RCT should be avoided. Similar to RCTs for colorectal tumors, heterogeneity in tumor stages should also be avoided [
23].
5. Conclusions
Robot-assisted hepatectomy has similar complication rates as the laparoscopic or open approaches. Major complications may be lower in RAH compared to LH, but more studies are needed to evaluate those in depth. Liver-specific complications have not shown to be reduced in RAH, and there is no evidence to support that patients with cirrhosis in particular should be favored for the robot-assisted approach.
Author Contributions
Conceptualization K.H.; methodology, A.M.-L. and J.F.; formal analysis A.M.-L.; investigation, J.F. and A.M.-L.; resources K.H.; data curation A.M.-L. and J.F.; writing—original draft preparation A.M.-L. and J.F.; writing—review and editing A.M.-L., J.F. and K.H.; visualization A.M.-L. and J.F.; supervision K.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data contributing to the analysis of this manuscript is available from the corresponding author upon reasonable request.
Acknowledgments
We thank Nicholas J. Murtha for the language review of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- George, E.I.; Brand, T.C.; LaPorta, A.; Marescaux, J.; Satava, R.M. Origins of Robotic Surgery: From Skepticism to Standard of Care. JSLS J. Soc. Laparoendosc. Surg. 2018, 22, e2018.00039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulchandani, J.; Shetty, N.; Kulkarni, A.; Shetty, S.; Sadat, M.S.; Kudari, A. Short-term and pathologic outcomes of robotic versus open pancreatoduodenectomy for periampullary and pancreatic head malignancy: An early experience. J. Robot. Surg. 2021. [Google Scholar] [CrossRef]
- Ayabe, R.I.; Azimuddin, A.; Tran Cao, H.S. Robot-assisted liver resection: The real benefit so far. Langenbeck’s Arch. Surg. 2022. [Google Scholar] [CrossRef]
- Shugaba, A.; Lambert, J.E.; Bampouras, T.M.; Nuttall, H.E.; Gaffney, C.J.; Subar, D.A. Should All Minimal Access Surgery Be Robot-Assisted? A Systematic Review into the Musculoskeletal and Cognitive Demands of Laparoscopic and Robot-Assisted Laparoscopic Surgery. J. Gastrointest. Surg. 2022. [Google Scholar] [CrossRef]
- Di Benedetto, F.; Petrowsky, H.; Magistri, P.; Halazun, K.J. Robotic liver resection: Hurdles and beyond. Int. J. Surg. 2020, 82, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Murtha-Lemekhova, A.; Fuchs, J.; Feiler, S.; Schulz, E.; Teroerde, M.; Kalkum, E.; Klotz, R.; Billeter, A.; Probst, P.; Hoffmann, K. Is metabolic syndrome a risk factor in hepatectomy? A meta-analysis with subgroup analysis for histologically confirmed hepatic manifestations. BMC Med. 2022, 20, 47. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Su, C.W.; Wei, C.Y.; Chau, G.Y.; Chen, P.H.; Chao, Y.; Huang, Y.H.; Wu, J.C.; Yang, T.C.; Lee, P.C.; et al. Comparison of prognoses between cirrhotic and non-cirrhotic patients with hepatocellular carcinoma and esophageal varices undergo surgical resection. J. Chin. Med. Assoc. 2022, 85, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Cumpston, M.; Chandler, J.; Lasserson, T. Chapter III: Reporting the review. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2 (Updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 10 June 2022).
- Kalkum, E.; Klotz, R.; Seide, S.; Hüttner, F.J.; Kowalewski, K.-F.; Nickel, F.; Khajeh, E.; Knebel, P.; Diener, M.K.; Probst, P. Systematic reviews in surgery—Recommendations from the Study Center of the German Society of Surgery. Langenbeck’s Arch. Surg. 2021, 406, 1723–1731. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Foroutan, F.; Guyatt, G.; Zuk, V.; Vandvik, P.O.; Alba, A.C.; Mustafa, R.; Vernooij, R.; Arevalo-Rodriguez, I.; Munn, Z.; Roshanov, P.; et al. GRADE Guidelines 28: Use of GRADE for the assessment of evidence about prognostic factors: Rating certainty in identification of groups of patients with different absolute risks. J. Clin. Epidemiol. 2020, 121, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Balzano, E.; Bernardi, L.; Tincani, G.; Ghinolfi, D.; Melandro, F.; Bronzoni, J.; Meli, S.; Arenga, G.; Biancofiore, G.; Crocetti, L.; et al. Implementing a robotic liver resection program does not always require prior laparoscopic experience. Surg. Endosc. 2021, 36, 3317–3322. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.D.; Wu, C.Y.; Hu, R.H.; Chou, W.H.; Lai, H.S.; Liang, J.T.; Lee, P.H.; Wu, Y.M. Robotic Versus Open Hepatectomy for Hepatocellular Carcinoma: A Matched Comparison. Ann. Surg. Oncol. 2017, 24, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Duong, L.M.; Cai, H.; Shrubsole, M.J.; Bailey, C.E.; Idrees, K.; Shu, X.O. Outcomes of robotic-assisted liver surgery versus laparoscopic liver surgery for treatment of stage I hepatocellular carcinoma. Cancer 2022, 128, 762–769. [Google Scholar] [CrossRef]
- Lai, E.C.; Tang, C.N. Long-term Survival Analysis of Robotic Versus Conventional Laparoscopic Hepatectomy for Hepatocellular Carcinoma: A Comparative Study. Surg. Laparosc. Endosc. Percutan. Tech. 2016, 26, 162–166. [Google Scholar] [CrossRef]
- Lim, C.; Goumard, C.; Salloum, C.; Tudisco, A.; Napoli, N.; Boggi, U.; Azoulay, D.; Scatton, O. Outcomes after 3D laparoscopic and robotic liver resection for hepatocellular carcinoma: A multicenter comparative study. Surg. Endosc. 2021, 35, 3258–3266. [Google Scholar] [CrossRef]
- Magistri, P.; Tarantino, G.; Guidetti, C.; Assirati, G.; Olivieri, T.; Ballarin, R.; Coratti, A.; Di Benedetto, F. Laparoscopic versus robotic surgery for hepatocellular carcinoma: The first 46 consecutive cases. J. Surg. Res. 2017, 217, 92–99. [Google Scholar] [CrossRef]
- Pesi, B.; Bencini, L.; Moraldi, L.; Tofani, F.; Batignani, G.; Bechi, P.; Farsi, M.; Annecchiarico, M.; Coratti, A. Robotic Versus Open Liver Resection in Hepatocarcinoma: Surgical and Oncological Outcomes. Surg. Laparosc. Endosc. Percutan. Tech. 2021, 31, 468–474. [Google Scholar] [CrossRef]
- Wang, W.H.; Kuo, K.K.; Wang, S.N.; Lee, K.T. Oncological and surgical result of hepatoma after robot surgery. Surg. Endosc. 2018, 32, 3918–3924. [Google Scholar] [CrossRef]
- Mohan, A.; Wara, U.U.; Arshad Shaikh, M.T.; Rahman, R.M.; Zaidi, Z.A. Telesurgery and Robotics: An Improved and Efficient Era. Cureus 2021, 13, e14124. [Google Scholar] [CrossRef]
- Rana, R.; Gaur, P.; Agarwal, V.; Parthasarathy, H. Tremor Estimation and Removal in Robot-Assisted Surgery Using Lie Groups and EKF. Robotica 2019, 37, 1904–1921. [Google Scholar] [CrossRef]
- Kim, M.J.; Park, S.C.; Park, J.W.; Chang, H.J.; Kim, D.Y.; Nam, B.H.; Sohn, D.K.; Oh, J.H. Robot-assisted Versus Laparoscopic Surgery for Rectal Cancer: A Phase II Open Label Prospective Randomized Controlled Trial. Ann. Surg. 2018, 267, 243–251. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}