
Health Outcomes of Exposure to Biological and Chemical Components of Inhalable and Respirable Particulate Matter


Abstract
:1. Introduction
2. Methods
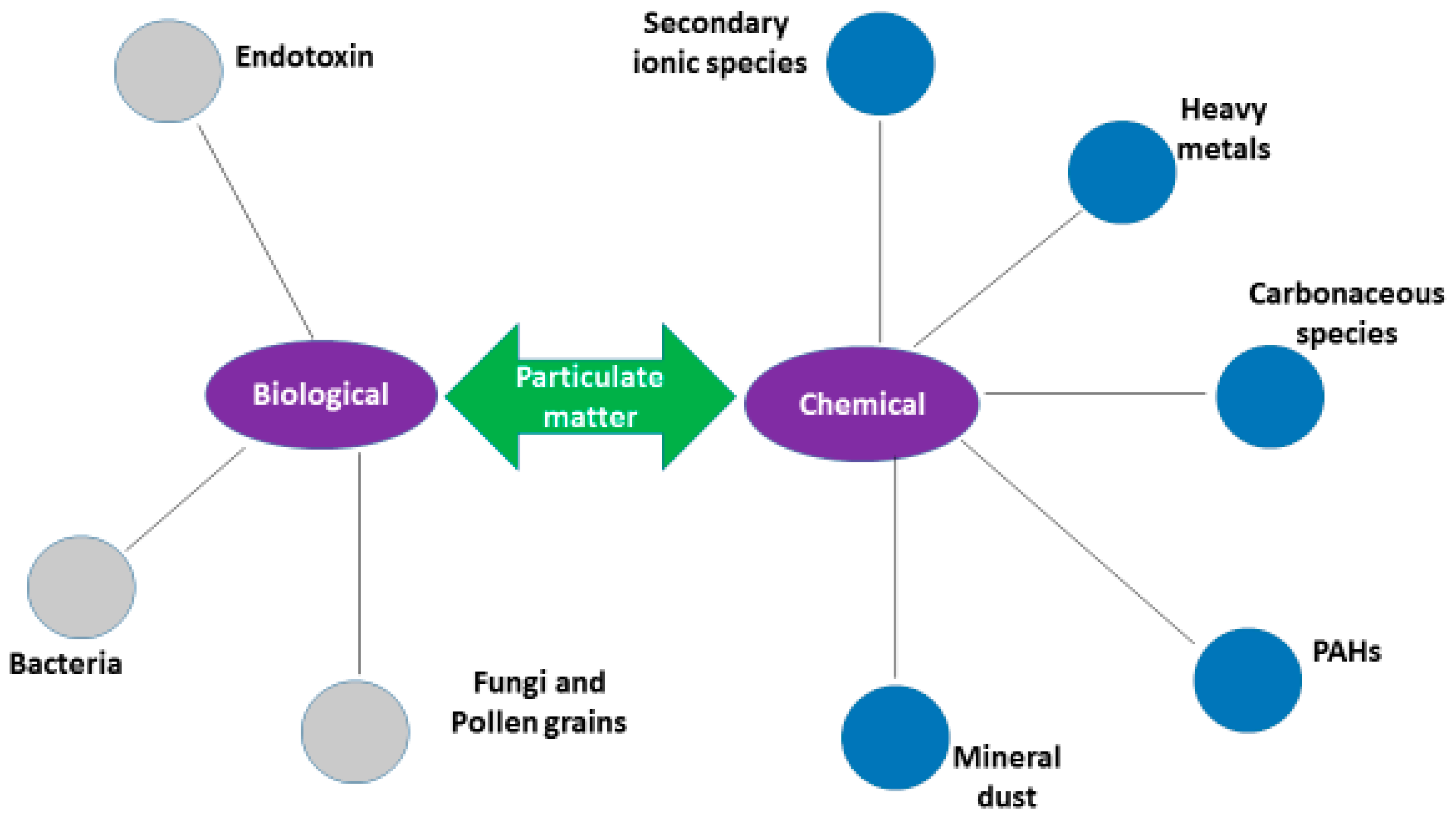
3. Particulate Matter-Associated Bioaerosols
3.1. Particulate Matter-Associated Endotoxins
3.2. Particulate Matter-Associated Bacteria
3.3. Particulate Matter-Associated Fungi and Pollen Grains
4. Chemicals in Airborne Particulate Matter
4.1. Particulate Matter-Associated Trace Metals
4.2. Particulate Matter-Associated Polycyclic Aromatic Hydrocarbons
4.3. Particulate Matter-Associated Inorganic Water Soluble Ionic Species
4.4. Particulate Matter-Associated Inorganic Mineral Dust
4.5. Particulate Matter-Associated Carbonaceous Species
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gilmour, M.I.; Koren, H.S. Interaction of inhaled particles with the immune system. In Particle–Lung Interactions. Lung Biology in Health and Disease; Gehr, P., Heyder, J., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2000; Volume 143, pp. 629–647. [Google Scholar]
- WHO. Ambient (Outdoor) Air Quality and Health. Available online: http://www.who.int/mediacentre/factssheet/fs313/en/ (accessed on 25 February 2016).
- Brauer, M.; Amann, M.; Burnett, R.T.; Cohen, A.; Dentener, F.; Ezzati, M.; Henderson, S.B.; Krzyzanowski, M.; Martin, R.V.; Van Dingenen, R.; et al. Exposure assessment for estimation of the global burden of disease attributable to outdoor air pollution. Environ. Sci. Technol. 2012, 46, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Jahan, S.A.; Kabir, E.; Brown, R.J.C. A review of airborne polycyclic aromatic hydrocarbons (PAHs) and their human health effects. Environ. Int. 2013, 60, 71–80. [Google Scholar] [CrossRef] [PubMed]
- USEPA. Particulate Matter. 2012. Available online: http://www.epa.gov/airquality/particlepollution/ (accessed on 26 February 2016). [Google Scholar]
- Brunekreef, B.; Holgate, S.T. Air pollution and health. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- Kelly, F.J.; Fussell, J.C. Size, source and chemical composition as determinants of toxicity attributable to ambient particulate matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Brown, J.S.; Gordon, T.; Price, O.; Asgharian, B. Thoracic and respirable particle definitions for human health risk assessment. Particle Fibre Toxcicol. 2013, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Dongarrà, G.; Manno, E.; Varrica, D.; Lombardo, M.; Vultaggio, M. Study on ambient concentrations of PM10, PM10-2.5, PM2.5 and gaseous pollutants. Trace elements and chemical speciation of atmospheric particulates. Atmos. Environ. 2010, 44, 5244–5257. [Google Scholar] [CrossRef]
- Kim, E.; Hopke, P.K.; Pinto, J.P.; Wilson, W.E. Spatial variability of fine particle mass, components, and source contributions during the regional air pollution study in St. Louis. Environ. Sci. Technol. 2005, 39, 4172–4179. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Dominici, F.; Pastor-Barriuso, R.; Zeger, S.L.; Samet, J.M. Seasonal analyses of air pollution and mortality in 100 U.S. cities. Am. J. Epidemiol. 2005, 161, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Oeder, S.; Dietrich, S.; Weichenmeier, I.; Schober, W.; Pusch, G.; Jörres, R.A.; Schierl, R.; Nowak, D.; Fromme, H.; Behrendt, H.; et al. Toxicity and elemental composition of particulate matter from outdoor and indoor air of elementary schools in Munich, Germany. Indoor Air 2012, 22, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Haas, D.; Galler, H.; Luxner, J.; Zarfel, G.; Buzina, W.; Fried, H.; Marth, E.; Habib, J.; Reinthaler, F.F. The concentrations of culturable microorganisms in relation to particulate matter in urban air. Atmos. Environ. 2013, 65, 215–222. [Google Scholar] [CrossRef]
- Meklin, T.; Reponen, T.; Toivola, M.; Koponen, V.; Husman, T.; Hyvärinen, A.; Nevalainen, A. Size distributions of airborne microbes in moisture-damaged and reference school buildings of two construction types. Atmos Environ. 2002, 36, 6031–6039. [Google Scholar] [CrossRef]
- Terzi, E.; Argyropoulos, G.; Bougatioti, A.; Mihalopoulos, N.; Nikolaou, K.; Samara, C. Chemical composition and mass closure of ambient PM10 at urban sites. Atmos Environ. 2010, 44, 2231–2239. [Google Scholar] [CrossRef]
- Lin, C.; Chen, S.; Huang, K.; Lee, W.; Lin, W.; Liao, C.; Chaung, H.; Chiu, C. Water-soluble ions in nano/ultrafine/fine/coarse particles collected near a busy road and at a rural site. Environ. Pollut. 2007, 145, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.; Buczynska, A.; Walgraeve, C.; Delcloo, A.; Potgieter-Vermaak, S.; Grieken, R.; Demeestere, K.; Dewulf, J.; Langenhove, H.; Backer, H.; et al. Acute changes in pulse pressure in relation to constituents of particulate air pollution in elderly persons. Environ. Res. 2012, 117, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Ying, Z.; Harkema, J.; Sun, Q.; Rajagopalan, S. Epidemiological and experimental links between air pollution and Type 2 diabetes. Toxicol. Pathol. 2013, 41, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Meister, K.; Johansson, C.; Forsberg, B. Estimated short-term effects of coarse particles on daily mortality in Stockholm, Sweden. Environ. Health Perspect. 2012, 120, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Proietti, E.; Roosli, M.; Frey, U.; Latzin, P. Air pollution during pregnancy and neonatal outcome: A review. J. Aerosol. Med. Pulmonary Drug Deliv. 2013, 26, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Rückerl, R.; Schneider, A.; Breitner, S.; Cyrys, J.; Peters, A. Health effects of particulate air pollution: A review of epidemiological evidence. Inhal. Toxicol. 2011, 23, 555–592. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.S.; Balkhair, T. Air pollution and birth outcomes: A systematic review. Environ. Int. 2011, 37, 498–516. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; He, G.; Liu, Y.; Yin, P.; Li, Y.; Kan, H.; Fan, M.; Xue, A.; Fan, M. The associations between ambient air pollution and adult respiratory mortality in 32 major Chinese cities, 2006–2010. Environ. Res. 2015, 137, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, K.; MacNee, W. Potential mechanism of adverse pulmonary and cardiovascular effects of particulate air pollution (PM10). Int. J. Hyg. Environ. Health 2001, 203, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, M.I.; Jaakkola, M.S.; London, S.J.; Nel, A.E.; Rogers, C.A. How exposure to environmental tobacco smoke, outdoor air pollutants, and increased pollen burdens influences the incidence of asthma. Environ. Health Perspect. 2006, 114, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Jaenicke, R. Abundance of cellular material and proteins in the atmosphere. Science 2005, 308, 73. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, M.; Parappukkaran, S.; Morawska, L.; Hitchins, J.; Congrong, H.; Gilbert, D. A pilot investigation into associations between indoor airborne fungal and non-biological particle concentrations in residential houses in Brisbane. Sci. Total Environ. 2003, 312, 89–101. [Google Scholar] [CrossRef]
- Heikkienen, M.S.A.; Hjelmroos-Koski, M.K.; Haggblom, M.M.; Macher, J.M. Bioaerosols. In Aerosols Handbook; Ruzer, L.S., Harley, N.H., Eds.; CRC Press: Boca Raton, FL, USA, 2005; pp. 291–342. [Google Scholar]
- Stetzenbach, L.D. Introduction to aerobiology. In Manual of Environmental Microbiology; ASM Press: Washington, DC, USA, 1997; pp. 619–628. [Google Scholar]
- Boreson, J.; Dillner, A.M.; Peccia, J. Correlating bioaerosol load with PM2.5 and PM10cf concentrations: A comparison between natural desert and urban-fringe aerosols. Atmos. Environ. 2004, 38, 6029–6041. [Google Scholar] [CrossRef]
- Pillai, S.D.; Ricke, S.C. Bioaerosols from municipal and animal wastes: Background and contemporary issues. Can. J. Microbiol. 2002, 48, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.J. Dorland's Medical Dictionary; W.B. Saunders Co.: Philadelphia, PA, USA, 1988. [Google Scholar]
- Thompson, W.A.R. Black's Medical Dictionary, 3rd ed.; Adam and Charles Black: London, UK, 1981. [Google Scholar]
- Stanley, R.G.; Linskins, H.F. Pollen: Biology, Chemistry and Management; Springer-Verlag: Berlin, Germany, 1974. [Google Scholar]
- Gregory, P.H. The Microbiology of the Atmosphere, 2nd ed.; Leonard Hall: Aylesbury, UK, 1973. [Google Scholar]
- Bauer, H.; Claeys, M.; Vermeylen, R.; Schueller, E.; Weinke, G.; Berger, A.; Puxbaum, H. Arabitol and mannitol as tracers for a quantification of airborne fungal spores. Atmos. Environ. 2008, 42, 588–593. [Google Scholar] [CrossRef]
- Menetrez, M.Y.; Foarde, K.K.; Webber, T.D.; Dean, T.R.; Betancourt, D.A. An evaluation of the protein mass of particulate matter. Atmos. Environ. 2007, 41, 8264–8274. [Google Scholar] [CrossRef]
- Womiloju, T.O.; Miller, J.D.; Mayer, P.M.; Brook, J.R. Methods to determine the biological composition of particular matter collected from outdoor air. Atmos. Environ. 2003, 37, 4335–4344. [Google Scholar] [CrossRef]
- D’Amato, G. Environmental urban factors (air pollution and allergens) and the rising trends in allergic respiratory diseases. Allergy 2002, 57, S30–S33. [Google Scholar] [CrossRef]
- Monn, C. Exposure assessment of air pollutants: A review on spatial heterogeneity and indoor/outdoor/personal exposure to suspended particulate matter, nitrogen dioxide and ozone. Atmos. Environ. 2001, 35, 1–32. [Google Scholar] [CrossRef]
- Lierl, M.B.; Hornung, R.W. Relationship of outdoor air quality to pediatric asthma exacerbations. Ann. Allergy Asthma Immunol. 2003, 90, 28–33. [Google Scholar] [CrossRef]
- Adhikari, A.; Reponen, T.; Grinshpun, S.A.; Martuzevicius, D.; LeMasters, G. Correlation of ambient inhalable bioaerosols with particulate matter and ozone: A two-year study. Environ. Pollut. 2006, 140, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Husman, T. Health effects of indoor-air microorganisms. Scand. J. Work Environ. Health 1996, 22, 5–13. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Thorne, P.S.; Yagla, S.J.; Burnmeister, L.F.; Denchuck, S.A.; Watt, J.L. The role of endotoxin in grain dust induced lung disease. A J. Respir. Crit. Care Med. 1995, 152, 503–600. [Google Scholar] [CrossRef] [PubMed]
- Targonski, P.; Persky, V.; Rameskrishnan, V. Effect of environmental moulds on risk of death from asthma during the pollen season. J. Allergy Clin. Immunol. 1995, 95, 955–961. [Google Scholar] [CrossRef]
- Beutler, B.; Rietschel, E.T. Innate immune sensing and its roots: The story of endotoxin. Nat. Rev. Immunol. 2003, 3, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Bartlett, K.; Graham, M.; Jackson, P. Ambient concentrations of airborne endotoxin in two cities in the interior of British Columbia. Can. J. Environ. Monit. 2011, 13, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, S.; Merritt, A.S.; Bellander, T. Endotoxins in urban air in Stockholm, Sweden. Atmos. Environ. 2011, 45, 266–270. [Google Scholar] [CrossRef]
- Carty, C.L.; Gehring, U.; Cyrys, J.; Bischof, W.; Heinrich, J. Seasonal variability of endotoxin in ambient fine particulate matter. J. Environ. Monit. 2003, 5, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Anneling, L.; Avol, J.M.P.; Thorne, P.S. Ambient endotoxin concentrations in PM10 from Southern California. Environ. Health Perspect. 2004, 112, 583. [Google Scholar] [CrossRef] [PubMed]
- Tager, I.B.; Lurmann, F.W.; Haight, T.; Alcorn, S.; Penfold, B.; Hammond, S.K. Temporal and spatial patterns of ambient endotoxin concentrations in Fresno, California. Environ. Health Perspect. 2010, 118, 1490–1496. [Google Scholar] [CrossRef] [PubMed]
- Monn, C.; Koren, H.S. Bioaerosols in ambient air particulates: A review and research needs. Environ. Health 1999, 14, 79–89. [Google Scholar] [CrossRef]
- Abbing-Karahagopian, V.; van der Gugten, A.C.; van der Ent, C.K.; Uiterwaal, C.; de Jongh, M.; Oldenwening, M.; Brunekreef, B.; Gehring, U. Effect of endotoxin and allergens on neonatal lung function and infancy respiratory symptoms and eczema. Pediatr. Allergy Immunol. 2012, 23, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Bolte, G.; Bischof, W.; Borte, M.; Lehmann, I.; Wichmann, H.E.; Heinrich, J.; LISA Study Group. Early endotoxin exposure and atopy development in infants: Results of a birth cohort study. Clin. Exp. Allergy 2003, 33, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Liebers, V.; Raulf-Heimsoth, M.; Brüning, T. Health effects due to endotoxin inhalation (review). Arch. Toxicol. 2008, 82, 203–210. [Google Scholar] [PubMed]
- Rabinovitch, N.; Liu, A.H.; Zhang, L.; Rodes, C.E.; Foarde, K.; Dutton, S.J.; Murphy, J.R.; Gelfand, E.W. Importance of the personal endotoxin cloud in school-age children with asthma. J. Allergy Clin. Immunol. 2005, 116, 1053–1057. [Google Scholar] [PubMed]
- Loh, L.C.; Vyas, B.; Kanabar, V.; Kemeny, D.M.; O’Connor, B.J. Inhaled endotoxin in healthy human subjects, A dose-related study on systemic effects and peripheral CD4þ and CD8þ T cells. Respir. Med. 2006, 100, 519–528. [Google Scholar] [PubMed]
- Thorn, J. The inflammatory response in humans after inhalation of bacterial endotoxin: A review. Inflammation 2001, 50, 254–261. [Google Scholar]
- Guastadisegni, C.; Kelly, F.J.; Cassee, F.R.; Gerlofs-Nijland, M.E.; Janssen, N.A.H.; Pozzi, R.; Brunekreef, B.; Sandstorm, T.; Mudway, I.S. Determinants of the pro-inflammatory action of ambient particulate matter in immortalised murine macrophages. Environ. Health Perspect. 2010, 118, 1728–1734. [Google Scholar] [PubMed]
- Shang, Y.; Zhu, T.; Lenz, A.G.; Frankenberger, B.; Tian, F.; Chen, C.; Stoeger, T. Reduced in vitro toxicity of fine particulate matter collected during the 2008 summer Olympic Games in Beijing: The roles of chemical and biological components. Toxicol. In Vitro 2013, 27, 2084–2093. [Google Scholar] [CrossRef] [PubMed]
- Alexis, N.E.; Lay, J.C.; Zeman, K.; Bennett, W.E.; Peden, D.B.; Soukup, J.M.; Devlin, R.B.; Becker, S. Biological material on inhaled coarse fraction particulate matter activates airway phagocytes in vivo in healthy volunteers. J. Allergy Clin. Immunol. 2006, 117, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Degobbi, C.; Hila, P. Endotoxin as modifier of particulate matter toxicity: A review of the literature. Aerobiol 2011, 27, 97–105. [Google Scholar] [CrossRef]
- Osornio-Vargas, A.R.; Bonner, J.C.; Alfaro-Moreno, E.; Martínez, L.; García-Cuellar, C.; Rosales, S.P.; Miranda, J.; Rosas, I. Pro-inflammatory and cytotoxic effects of Mexico city air pollution particulate matter in vitro are dependent on particle size and composition. Environ. Health Perspect. 2003, 111, 1289. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.H.; Bernstein, D.I.; Lockey, J.; Reponen, T.; Levin, L.; Grinshpun, S.; Villareal, M.; Hershey, G.K.K.; Burkle, J.; LeMasters, G. Exposure to traffic related particles and endotoxin during infancy is associated with wheezing at age 3 years. Am. J. Respir. Crit. Care Med. 2009, 180, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Monn, C.; Becker, S. Cytotoxicity and induction of proinflammatory cytokines from human monocytes exposed to fine (PM2.5) and coarse particles (PM10-2.5) in outdoor and indoor air. Toxicol. Appl. Pharmacol. 1999, 155, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Ning, Y.; Imrich, A.; Goldsmith, C.A.; Qin, G.; Kobzik, L. Alveolar macrophage cytokine production in response to air particles in vitro: Role of endotoxin. J. Toxicol. Environ. Health 2000, 59, 165–180. [Google Scholar]
- Gangamma, S. Airborne particulate matter associated endotoxin and proinflammatory responses. J. Allergy Clin. Immunol. 2012, 130, 1012–1013. [Google Scholar] [CrossRef] [PubMed]
- Bowers, R.M.; Sullivan, A.P.; Costello, E.K.; Collett, J.L., Jr.; Knight, R.; Fierer, N. Sources of bacteria in outdoor air across cities in the Midwestern United States. Appl. Environ. Microbiol. 2011. [Google Scholar] [CrossRef] [PubMed]
- Brodie, E.L.; DeSantis, T.Z.; Parker, J.P.M.; Zubietta, I.X.; Piceno, Y.M.; Andersen, G.L. Urban aerosols harbourharbor diverse and dynamic bacterial populations. Proc. Natl. Acad. Sci. USA 2007, 104, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Elbert, W.; Taylor, P.E.; Andreae, M.O.; P¨oschl, U. Contribution of fungi to primary biogenic aerosols in the atmosphere: Wet and dry discharged spores, carbohydrates, and inorganic ions. Atmos. Chem. Phys. 2007, 7, 4569–4588. [Google Scholar] [CrossRef]
- Fang, Z.G.; Ouyang, Z.Y.; Zheng, H.; Wang, X.K.; Hu, L.F. Culturable airborne bacteria in outdoor environments in Beijing, China. Microb. Ecol. 2007, 54, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, B.T.; Lighthart, B. Survey of culturable airborne bacteria at four diverse locations in Oregon: Urban, rural, forest, and coastal. Microb. Ecol. 1997, 34, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Maron, P.A.; Mougel, C.; Lejon, D.P.H.; Carvalho, E.; Bizet, K.; Marck, G.; Cubito, N.; Lemanceau, P.; Ranjard, L. Temporal variability of airborne bacterial community structure in an urban area. Atmos. Environ. 2006, 40, 8074–8080. [Google Scholar] [CrossRef]
- Polymenakou, P.N.; Mandalakis, M.; Stephanou, E.G.; Tselepides, A. Particle size distribution of airborne microorganisms and pathogens during an intense African dust event in the Eastern Mediterranean. Environ. Health Perspect. 2008, 116, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Frohlich-Nowoisky, J.; Pickersgill, D.A.; Despres, V.R.; Poschl, U. High diversity of fungi in air particulate matter. Proc. Natl. Acad. Sci. USA 2009, 106, 12814–12819. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Engling, G.; Chan, C.; Zhang, Y.; Zhang, Z.; Lin, M.; Xue-Fang, S.X.; Li, Y.D.; Li, Y. Contribution of fungal spores to particulate matter in a tropical rainforest. Environ. Res. Lett. 2010, 5. [Google Scholar] [CrossRef]
- Glikson, M.; Rutherford, S.; Simpson, R.W.; Mitchel, L.C.A.; Yago, A. Microscopic and submicron components of atmospheric particulate matter during high asthma periods in Brisbane, Queensland, Australia. Atmos. Environ. 1995, 29, 549–562. [Google Scholar] [CrossRef]
- Kendrick, B. Fungal Allergens Sampling and Identifying Allergenic Pollens and Moulds; Smith, E.G., Ed.; Blewstone Press: San Antonio, CA, USA, 1990; pp. 134–164. [Google Scholar]
- Risse, U.; Tomczok, J.; Huss-Marp, J.; Darsow, U.; Behrendt, H. Health-relevant interaction between airborne particulate matter and aeroallergens (pollen). J. Aerosol. Sci. 2000, 31, S27–S28. [Google Scholar] [CrossRef]
- Cakmak, S.; Dales, R.E.; Burnett, R.T.; Judek, S.; Coates, F.; Brook, J.R. Effects of airborne allergens on emergency visits by children for conjunctivitis and rhinitis. Lancet 2002, 359, 947–948. [Google Scholar] [CrossRef]
- Adhikari, A.; Sen, M.M.; Gupta-Bhattacharya, S.; Chanda, S. Airborne viable, non-viable, and allergenic fungi in a rural agricultural area of India: A 2-year study at five outdoor sampling stations. Sci. Total Environ. 2004, 326, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Bush, R.K.; Portnoy, J.M. The role and abatement of fungal allergens in allergic diseases. J. Allergy Clin. Immunol. 2001, 107, S430–S440. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.E.; Cakmak, S.; Judek, S.; Dann, T.; Coates, F.; Brook, J.R.; Burnett, R.T. The role of fungal spores in thunderstorm asthma. Chest 2003, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.A. Update on airborne mould and mould allergy. Allergy Asthma Proc. 1999, 20, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Solomon, W.R. Airborne pollen: A brief life. J. Allergy Clin. Immunol. 2002, 109, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Hasnain, S.M.; Al-Frayh, A.S.; Al-Suwaine, A.; Gad-El-Rab, M.O.; Fatima, K.; Al-Sedairy, S. Cladosporium and respiratory allergy: Diagnostic implications in Saudi Arabia. Mycopathologia 2004, 157, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Raes, F.; Van Dingenen, R.; Vignati, E.; Wilson, J.; Putaud, J.P.; Seinfeld, J.H.; Adams, P. Formation and cycling of aerosols in the global troposphere. Atmos. Environ. 2000, 34, 4215–4240. [Google Scholar] [CrossRef]
- Williams, J.; de Reus, M.; Krejci, R.; Fischer, H.; Strom, J. Application of the variability-size relationship to atmospheric aerosol studies: Estimating aerosol lifetimes and ages. Atmos. Chem. Phys. 2002, 2, 133–145. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Samet, J.M.; Dominici, F. Hospital admissions and chemical composition of fine particle air pollution. Am. J. Respir. Crit. Care Med. 2009, 12, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Bell, M.L.; Geyh, A.S.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Emergency admissions for cardiovascular and respiratory diseases and the chemical composition of fine particle air pollution. Environ. Health Perspect. 2009, 117, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.; Feng, W.Y.; Broadwin, R.; Green, S.; Lipsett, M. The effects of components of fine particulate air pollution on mortality in California: Results from CALFINE. Environ. Health Perspect. 2007, 115, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Franklin, M.; Koutrakis, P.; Schwartz, J. Fine particulate air pollution and its components in association with cause-specific emergency admissions. Environ. Health 2009, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Franklin, M.; Koutrakis, P.; Schwartz, J. The role of particle composition on the association between PM2.5 and mortality. Epidemiology 2008, 19, 680–689. [Google Scholar] [CrossRef]
- Bell, M.L.; Belanger, K.; Ebisu, K.; Gent, J.F.; Lee, H.J.; Koutrakis, P.; Leaderer, B.P. Prenatal exposure to fine particulate matter and birth weight: Variations by particulate constituents and sources. Epidemiology 2010, 21, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B. The colour of smoke. Epidemiology 2010, 21, 903–904. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Wiedinmyer, C.; Baker, K.R.; Hannigan, M.P. Characterization of coarse particulate matter in the western United States: A comparison between observation and modeling. Atmos. Chem. Phys. Discuss 2012, 12, 11445–11484. [Google Scholar] [CrossRef]
- Shang, Z.; Cheng, L.; Yu, Q.; He, L.; Lu, Z. Changing characteristics on dust storm in Jiangsu. Open J. Air Pollut. 2012, 1, 67–73. [Google Scholar] [CrossRef]
- Wang, Y.; Hopke, P.K.; Chalupa, D.C.; Utell, M.J. Effect of the shutdown of a coal-fired power plant on urban ultrafine particles and other pollutants. Aerosol Sci. Tech. 2011, 45, 1245–1249. [Google Scholar] [CrossRef]
- Schlesinger, R.B.; Kunzli, N.; Hidy, G.M.; Gotschi, T.; Jerrett, M. The health relevance of ambient particulate matter characteristics: Coherence of toxicological and epidemiological inferences. Inhal. Toxicol. 2006, 18, 95–125. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Committee on the Medical Effects of Air Pollutants: Asthma and Outdoor Air Pollutants; HMSO: London, UK, 1995. [Google Scholar]
- Diaz, R.V.; Dominguez, E.R. Health risk by inhalation of PM (2.5) in the metropolitan zone of the City of Mexico. Ecotox Environ. Safety 2009, 72, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Gavett, S.H.; Koren, H.S. The role of particulate matter in exacerbation of atopic asthma. Int. Arch. Immunol. 2001, 124, 109–112. [Google Scholar] [CrossRef]
- Boffetta, P.; Jourenkova, N.; Gustavsson, P. Cancer risk from occupational and environmental exposure to polycyclic aromatic hydrocarbons. Cancer Causes Control 1997, 8, 444–472. [Google Scholar] [CrossRef] [PubMed]
- Perera, F.; Rauh, V.; Tsai, W.Y.; Kinney, P.; Camann, D.; Barr, D.; Bernert, T.; Garfinkel, R.; Tu, Y.; Diaz, D.; et al. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multiethnic population. Environ. Health Perspect. 2003, 111, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.C.; Jedrychowski, W.; Butscher, M.; Camann, D.; Kieltyka, A.; Mroz, E.; Flak, E.; Li, Z.; Wang, S.; Rauh, V. Prenatal exposure to airborne polycyclic aromatic hydrocarbons and children’s intelligence at 5 years of age in a prospective cohort study in Poland. Environ. Health Perspect. 2010, 118, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.T.; Dales, R.; Krewski, D.; Vincent, R.; Dann, T.; Brook, J.R. Associations between ambient particulate sulfate and admissions to Ontario hospitals for cardiac and respiratory diseases. Am. J. Epidemiol. 1995, 142, 15–22. [Google Scholar] [PubMed]
- Delfino, R.J.; Murphy-Moulton, A.M.; Burnett, R.T.; Brook, J.R.; Becklake, M.R. Effects of air pollution on emergency room visits for respiratory illnesses in Montreal, Quebec. Am. J. Respir. Crit. Care Med. 1997, 155, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Bennet, C.M.; McKendry, I.G.; Kelly, S.; Denike, K.; Koch, T. Impact of the 1998 Gobi dust event on hospital admissions in the lower Fraser Valley, British Columbia. Sci. Total Environ. 2006, 366, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.C.; Rice, A.B.; Lindroos, P.M.; O’Brian, P.O.; Dreher, K.L.; Rosas, I. Introduction of the lung myofibroblast PDGF receptor system by urban ambient particles from Mexico city. Am. J. Resp. Cell Mol. Biol. 1998, 19, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.W.; Luttman-Gibson, H.; Rich, D.Q.; Link, M.S.; Mittleman, M.A.; Gold, D.R.; Koutrakis, P.; Schwartz, J.D.; Verrier, R.L. Association of air pollution with increased incidence of ventricular tachyarrhythmias recorded by implanted cardioverter defibrillators. Environ. Health Perspect. 2005, 113, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Frampton, M.W.; Ghio, A.J.; Samet, J.M.; Carson, J.L.; Carter, J.D.; Devlin, R.B. Effects of aqueous extracts of PM10 filters from the Utah Valley on human airway epithelial cells. Am. J. Phys. 1999, 277, L970–L967. [Google Scholar]
- Ghio, A.J.; Kim, C.; Devlin, R.B. Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. Am. J. Respir. Crit. Care Med. 2000, 162, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.I.; Ito, K.; Lippmann, M. Effects of thoracic and fine PM and their components on heart rate and pulmonary function and COPD patients. J. Exp. Sci. Environ. Med. 2011, 21, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Lall, R.; Ito, K.; Thurston, G.D. Distributed lag analyses of daily admissions and source-apportioned fine particle air pollution. Environ. Health Perspect. 2011, 119, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Strickland, J.; Lyndsey, A.; Darrow, M.; Klein, M.; Flanders, W.D.; Sarnet, J.A.; Waller, L.A.; Sarnat, S.E.; Mulholland, J.A.; Tolbert, P.E. Short-term associations between ambient air pollutants and pediatric asthma emergency department visits. Am. J. Respir. Crit. Care Med. 2010, 182, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Thurston, G.D.; Ito, K.; Hayes, C.G.; Bates, D.V.; Lippmann, M. Respiratory hospital admissions and summertime haze air pollution in Toronto, Ontario: Consideration of the role of acid aerosols. Environ. Res. 1994, 65, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Wellenius, G.A.; Burger, M.R.; Coull, B.A.; Schwartz, J.; Suh, H.H.; Koutrakis, P.; Schlaug, G.; Gold, D.R.; Mittlemen, M.A. Ambient air pollution and the risk of acute ischemic stroke. Arch. Intern. Med. 2012, 172, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ito, K.; Lall, R.; Lippman, M.; Thurston, G. Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ. Health Perspect. 2011, 119, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Samara, C.; Voutsa, D. Size distribution of airborne particulate matter and associated heavy metals in the roadside environment. Chemosphere 2005, 59, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Pacyna, J.M. Toxic Metals in the Atmospheres; Nriagu, J.O., Davidson, C.I., Eds.; Wiley: New York, NY, USA, 1986; pp. 2–32. [Google Scholar]
- Hu, X.; Zhang, Y.; Ding, Z.; Wang, T.; Lian, H.; Sun, Y.; Wu, J. Bioaccessibility and health risk of arsenic and heavy metals (Cd, Co, Cr, Cu, Ni, Pb, Zn and Mn) in TSP and PM2.5 in Nanjing, China. Atmos. Environ. 2012, 57, 146–152. [Google Scholar] [CrossRef]
- Dye, J.A.; Lehman, J.R.; McGee, J.K.; Winset, D.W.; Ledbetter, A.D.; Everitt, J.I.; Ghio, A.J.; Costa, D. Acute pulmonary toxicity of particle matter filter extracts in rats coherence with epidemiologic studies in Utah Valley residents. Environ. Health Perspect. 2001, 109, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Sunm, G.; Crissman, K.; Norwood, J.; Richards, J.; Slade, R.; Hatch, G.E. Oxidative interactions of synthetic lung epithelial lining fluid with metal-containing particulate matter. Am. J. Physiol. Lung Cell Mol. Physiol. 2001, 281, 1807–1815. [Google Scholar]
- Graff, D.W.; Cascio, W.E.; Brackhan, J.A.; Devlin, R.B. Metal particulate matter components affect gene expression and beat frequency of neonatal rat ventricular myocytes. Environ. Health Perspect. 2004, 112, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Carter, J.D.; Dailey, L.A.; Huang, Y.C. Pollutant particles produce vasoconstriction and enhance MAPK signaling via angiotensin type I receptor. Environ. Health Perspect. 2005, 113, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Costa, X.; Dreher, X. Bioavailable transition metals in particulate matter mediate cardiopulmonary injury in healthy and compromised animal models. Environ. Health Perspect. 1997, 105, S1053–S1060. [Google Scholar] [CrossRef]
- Manalis, N.; Grivas, G.; Protonotarios, V.; Moutsatsou, A.; Samara, C.; Chaloulakou, A. Toxic metal content of particulate matter (PM10), within the Greater Area of Athens. Chemosphere 2005, 60, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Ambient Air Pollution by As, Cd and Ni Compounds—Position Paper. Available online: http://ec.europa.eu/environment/archives/air/pdf/pp_as_cd_ni.pdf (accessed on 13 June 2016).
- WHO. Air Quality Guidelines, 2nd ed.; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Campen, M.J.; Nolan, J.P.; Schladweiler, M.C.J.; Kodavanti, U.P.; Evansky, P.A.; Costa, D.L.; Watkinson, W.P. Cardiovascular and thermoregulatory effects of inhaled PM-associated transition metals: A potential interaction between nickel and vanadium sulfate. Toxicol. Sci. 2001, 64, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Jianjun, N.; Rasmussen, P.E.; Hassan, N.M.; Vincent, R. Concentration distribution and bioaccessibility of trace elements in Nano and fine urban airborne particulate matter: Influence of particle size. Water Air Soil Pollut. 2010, 213, 211–225. [Google Scholar]
- Song, S.; Lee, K.; Lee, Y.M.; Lee, J.H.; Lee, S.; Yu, S.D.; Paek, D. Acute health effects of urban fine and ultrafine particles on children with atopic dermatitis. Environ. Res. 2011, 3, 394–399. [Google Scholar] [CrossRef] [PubMed]
- CCME (Canadian Council of Ministers of the Environment). Canadian Soil Quality Guidelines for Potentially Carcinogenic and Other Pahs: Scientific Criteria Document; CCME: Winnipeg, MB, Canada, 2010. [Google Scholar]
- Kim, K.H.; Jahan, S.A.; Kabir, E. A review on human health perspective of air pollution with respect to allergies and asthma. Environ. Int. 2013, 59, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Masih, J.; Singhvi, R.; Kumar, K.; Jain, V.K.; Taneja, A. Seasonal variation and sources of polycyclic aromatic hydrocarbons (PAHs) in indoor and outdoor air in a semi-arid tract of Northern India. Aerosol. Air Qual. Res. 2012, 12, 515–525. [Google Scholar] [CrossRef]
- Lee, R.G.M.; Coleman, P.; Jones, J.L.; Jones, K.C.; Lohmann, R. Emission factors and importance of PCDD/Fs, PCBs, PCNs, PAHs and PM10 from the domestic burning of coal and wood in the UK. Environ. Sci. Technol. 2005, 39, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Jain, V.K.; Khan, Z.H. Characterization and source identification of polycyclic aromatic hydrocarbons (PAHs) in the urban environment of Delhi. Chemosphere 2007, 66, 302–310. [Google Scholar] [CrossRef] [PubMed]
- WHO. Polynuclear Aromatic Hydrocarbons in Drinking-Water. Background Document for Development of WHO Guidelines for Drinking-water Quality; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Akyuz, M.; Cabuk, H. Gas-particle partitioning and seasonal variation of polycyclic aromatic hydrocarbons in the atmosphere of Zonguldak, Turkey. Sci. Total Environ. 2010, 408, 5550–5558. [Google Scholar] [CrossRef] [PubMed]
- Fang, G.C.; Wu, Y.S.; Chen, J.C.; Chang, C.N.; Ho, T.T. Characteristic of polycyclic aromatic hydrocarbon concentrations and source identification for fine and coarse particulates at Taichung Harbor near Taiwan Strait during 2004–2005. Sci. Total Environ. 2006, 366, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.P.; Tao, S.; Liu, W.X. Particle size distributions of polycyclic aromatic hydrocarbons in rural and urban atmosphere of Tianjin, China. Chemosphere 2006, 62, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Saborit, J.M.; Aquilina, N.; Baker, S.; Harrad, S.; Meddings, C.; Harrison, R.M. Determination of atmospheric particulate-phase polycyclic aromatic hydrocarbons from low volume air samples. Anal. Meth. 2010, 2, 231–242. [Google Scholar] [CrossRef]
- Wang, Z.; Ren, P.; Sun, Y.; Ma, X.; Liu, X.; Na, G.; Yao, Z. Gas/particle partitioning of polycyclic aromatic hydrocarbons in coastal atmosphere of the north Yellow Sea. Environ. Sci. Pollut. Res. 2013, 20, 5753–5763. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.M.G.; Tsay, L.-Y. The partitioning model of polycyclic aromatic hydrocarbon between gaseous and particulate (PM10A) phases in urban atmosphere with high humidity. Sci. Total Environ. 1994, 145, 163–171. [Google Scholar] [CrossRef]
- Pankow, J.F.; Bidleman, T.F. Effects of temperature, TSP, and percent non-exchangeable material in determining the gas–particle partitioning of organic compounds. Atmos. Environ. 1999, 25, 2241–2249. [Google Scholar] [CrossRef]
- Finlayson-Pitts, B.; Pitts, J.N. Tropospheric air pollution: Ozone, airborne toxics an polycyclic aromatic hydrocarbons and particles. Science 1997, 276, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, C.; FriedIander, S. Size distributions of polycyclic aromatic hydrocarbons and elemental carbon: Ambient measurement and effects of atmospheric processes. Environ. Sci. Tech. 1994, 28, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, M.; Çabuk, H. Particle-associated polycyclic aromatic hydrocarbons in the atmospheric environment of Zonguldak, Turkey. Sci. Total Environ. 2008, 405, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Skarek, M.; Janosek, J.; Cupr, P.; Kohoutek, J.; Novotna-Rychetska, A.; Holoubek, I. Evaluation of genotoxic and non-genotoxic effects of organic air pollution using in vitro bioassays. Environ. Int. 2007, 33, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Gilli, G.; Pignata, C.; Schiliro, T.; Bono, R.; Rosa, A.L.; Traversi, D. The mutagenic hazards of environmental PM2.5 in Turin. Environ. Res. 2007, 103, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Oanh, N.H.K.; Reutergardh, L.B.; Dung, N.T. Emission of polycyclic aromatic hydrocarbons and particulate matter from domestic combustion of selected fuels. Environ. Sci. Technol. 1999, 33, 2703–2709. [Google Scholar] [CrossRef]
- Armstrong, B.G.; Hutchinson, E.; Unwin, J.; Fletcher, T. Lung cancer risk after exposure to polycyclic aromatic hydrocarbons: A review and meta-analysis. Environ. Health Perspect. 2004, 112, 970–978. [Google Scholar] [CrossRef] [PubMed]
- ACGIH (American Conference of Governmental Industrial Hygienists). Polycyclic Aromatic Hydrocarbons (PAHs) Biologic Exposure Indices (BEI) Cincinnati; American Conference of Governmental Industrial Hygienists: Cincinnati, OH, USA, 2005. [Google Scholar]
- Unwin, J.; Cocker, J.; Scobbie, E.; Chambers, H. An assessment of occupational exposure to polycyclic aromatic hydrocarbons in the UK. Ann. Occup. Hyg. 2006, 50, 395–403. [Google Scholar] [CrossRef] [PubMed]
- ATSDR (Agency for Toxic Substances, Disease Registry). Toxicological Profile for Polycyclic Aromatic Hydrocarbons; U.S. Department of Health and Human Services, U.S. Government Printing Office: Washington, DC, USA, 1995; pp. 639–298. [Google Scholar]
- Srogi, K. Monitoring of environmental exposure to polycyclic aromatic hydrocarbons: A review. Environ. Chem. 2007, 5, 169–195. [Google Scholar] [CrossRef]
- Garcia-Suastegui, W.A.; Huerta-Chagoya, A.; Carrasco-Colın, K.L.; Pratt, M.M.; John, K.; Petrosyan, P.; Rubio, J.; Poirier, M.C.; Gonsebatt, M.E. Seasonal variations in the levels of PAH-DNA adducts in young adults living in Mexico city. Mutagenesis 2011, 26, 385–391. [Google Scholar] [CrossRef] [PubMed]
- John, K.; Ragavan, N.; Pratt, M.M.; Singh, P.B.; Al-Buheissi, S.; Matanhelia, S.S. Quantification of phase I/II metabolizing enzyme gene expression and polycyclic aromatic hydrocarbon-DNA adduct levels in human prostate. Prostate 2009, 69, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Hsu, Y.W.; Lee, H.S. Study of human exposure to particulate PAHs using personal air samplers. Arch. Environ. Contam. Toxicol. 2003, 44, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Perera, F.; Tang, D.; Whyatt, R.; Lederman, S.A.; Jedrychowski, W. DNA damage from polycyclic aromatic hydrocarbons measured by benzo(a)pyrene-DNA adducts in mothers and newborns from Northern Manhattan, the World Trade Center Area, Poland, and China. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Ormstad, H.; Johansen, B.V.; Gaarder, P.I. Airborne house dust particles and diesel exhaust particles as allergen carriers. Clin. Exp. Allergy 1998, 28, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Omar, N.Y.M.J.; Mon, T.C.; Rahman, N.A.; Abas, M.R.B. Distributions and health risks of polycyclic aromatic hydrocarbons (PAHs) in atmospheric aerosols of Kuala Lumpur, Malaysia. Sci. Total Environ. 2006, 369, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; Lin, J.; Yao, Y.; Hung, L.; Chiang, H. Size Distribution and water soluble ions of ambient particulate matter on episode and non-episode days in Southern Taiwan. Aerosol Air Qual. Res. 2012, 12, 263–274. [Google Scholar] [CrossRef]
- Deshmukh, D.K.; Deb, M.K.; Tsai, Y.I.; Mkoma, S.L. Water soluble ions in PM2.5 and PM1 aerosols in Durg city, Chhattisgarh, India. Aerosol Air Qual. Res. 2011, 11, 696–708. [Google Scholar] [CrossRef]
- Stone, E.A.; Yoon, S.C.; Schauer, J.J. Chemical characterization of fine and coarse particles in Gosan, Korea during Springtime Dust Events. Aerosol Air Qual. Res. 2011, 11, 31–43. [Google Scholar] [CrossRef]
- Zhao, Y.; Gao, Y. Mass size distributions of water-soluble inorganic and organic ions in size-segregated aerosols over Metropolitan Newark in the U.S. East Coast. Atmos. Environ. 2008, 42, 4063–4078. [Google Scholar] [CrossRef]
- Plaza, J.; Pujadas, M.; Gómez-Moreno, F.J. Sánchez, M.; Artíñano, B. Mass size distribution of soluble sulfate, nitrate and ammonium in the Madrid urban aerosol. Atmos. Environ. 2011, 45, 4966–4976. [Google Scholar] [CrossRef]
- Shen, Z.; Wang, X.; Zhang, R.; Ho, K.; Cao, J.; Zhang, M. Chemical composition of water-soluble ions and carbonate estimation in spring aerosol at a semiarid site of Tongyu, China. Aerosol Air Qual Res. 2011, 11, 360–368. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, F.; Xu, Y.; Chen, J.; Yin, L.; Shang, X.; Xu, L. Chemical characteristics of particulate matter during a heavy dust episode in a coastal city, Xiamen, 2010. Aerosol Air Qual. Res. 2011, 11, 299–308. [Google Scholar] [CrossRef]
- Ying, Q.; Kleeman, M.J. Source contributions to the regional distribution of secondary particulate matter in California. Atmos. Environ. 2006, 40, 736–752. [Google Scholar] [CrossRef]
- Han, Y.J.; Kim, T.S.; Kim, H. Ionic constituents and source analysis of PM2.5 in three Korea cities. Atmos. Environ. 2008, 42, 3127–3141. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A. Acute respiratory effects of particulate air pollution. Annul. Rev. Public Health 1994, 15, 107–132. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M.; Thurston, G.D. Sulfate concentrations as an indicator of ambient particulate matter air pollution for health risk evaluations. J. Expo. Anal Environ. Epidemiol. 1996, 6, 123–146. [Google Scholar] [PubMed]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.; Pope, A. Epidemiology of acute health effects: Summary of time-series studies. In Particles in Our Air: Concentrations and Health Effects; Wilson, R., Spengler, J., Eds.; Harvard University Press: Boston, MA, USA, 1996; pp. 123–147. [Google Scholar]
- Hoek, G.; Brunekreef, B. Effects of low level winter air pollution on respiratory health of Dutch children. Environ. Res. 1994, 64, 136–150. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A. Invited Commentary: Particulate matter-mortality exposure-response relations and threshold. Am. J. Epidemiol. 2000, 152, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Tobias, A.; Querol, X.; Kunzli, N.; Pey, J.; Alastuey, A.; Viana, M.; Valero, N.; Gonzales-Cabre, M.; Sunyer, J. Coarse particles from Saharan dust and daily mortality. Epidemiology 2007, 19, 800–807. [Google Scholar] [CrossRef]
- Hefflin, B.J.; Jalaludin, B.; McClue, E.; Cobb, N.; Johnson, C.A.; Jecha, L.; Etzel, R.A. Surveillance for dust storms and respiratory diseases in Washington State. Arch. Environ. Health 1994, 49, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, E.; Linares, C.; Martinez, D.; Diaz, J. Role of Saharan dust in the relationship between particulate matter and short-term daily mortality among the elderly in Madrid (Spain). Sci. Tot Environ. 2010, 408, 5729–5736. [Google Scholar] [CrossRef] [PubMed]
- Mallone, S.; Stafoggia, M.; Faustini, A.; Gobbi, G.P.; Marconi, A.; Forastiere, F. Saharan dust and associations between particulate matter and daily mortality in Rome, Italy. Environ. Health Perspect. 2011, 119. [Google Scholar] [CrossRef]
- Lopez-Villarrubia, E.; Ballaster, F.; Iniguez, C.; Peral, N. Air pollution and mortality in the Canary Islands: A time series analysis. Environ. Health 2010, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Prospero, J.M.; Blades, E.; Naidu, R.; Mathison, G.; Thani, H.; Lavoie, M.C. Relationship between African dust carried in the Atlantic trade winds and surges in pediatric asthma attendances in the Caribbean. Int. J. Biometeor. 2008, 52, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Shaocai, Y.u.; Robin, L.D.; Prakash, V.B.; Brian, K.E. Primary and secondary organic aerosols over the United States: Estimates on the basis of observed organic carbon (OC) and elemental carbon (EC), and air quality modeled primary OC/EC ratios. Atmos. Environ. 2004, 38, 5257–5268. [Google Scholar]
- Seinfeld, J.H.; Pandis, S.N. Atmospheric Chemistry and Physics: From Air Pollution to Climate Change; Wiley: New York, NY, USA, 1998. [Google Scholar]
- Malm, W.C.; Schichtel, B.A.; Pitchford, M.L.; Ashbaugh, L.L.; Eldred, R.A. Spatial and monthly trends in speciated fine particle concentration in the United States. J. Geophys. Res. Atmos. 2004, 109. [Google Scholar] [CrossRef]
- Putaud, J.P.; Raes, F.; van Dingenen, R.; Baltensperger, U.; Bru¨ggemann, E.; Facchini, M.C.; Decesari, S.; Fuzzi, S.; Gehrig, R.; Hansson, H.C.; et al. European Aerosol Phenomenology II: Chemical characteristics of particulate matter at kerbside, urban, rural and background sites in Europe. Atmos. Environ. 2004, 38, 2579–2595. [Google Scholar] [CrossRef]
- Querol, X.; Alastuey, A.; Rodríguez, S.; Viana, M.M.; Artíñano, B.; Salvador, P. Levels of PM in rural, urban and industrial sites in Spain. Sci. Total Environ. 2004, 334–335, 359–376. [Google Scholar] [CrossRef] [PubMed]
- Turpin, B.J.; Huntzicker, J.J. Identification of secondary organic aerosol episodes and quantitation of primary and secondary organic aerosol concentrations during SCAQS. Atmos. Environ. 1995, 29, 3527–3544. [Google Scholar] [CrossRef]
- Li, H.; Feng, J.; Sheng, G.; Lü, S.; Fu, J.; Peng, P.; Ren, M. The PCDD/F and PBDD/F pollution in the ambient atmosphere of Shanghai, China. Chemosphere 2008, 70, 576–583. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Type of Study | Study Population | Study Location | Pollutant Analyzed | Health Outcome |
|---|---|---|---|---|---|
| Schwartz et al. [44] | Cross-sectional | Grain handlers and postal workers | Iowa City | Endotoxin and grain dust | Concentration of endotoxin in the may be important in the development of grain dust-induced lung disease. |
| Targonski et al. [45] | Cross-sectional | 5- to 34-year-olds in the general population 1985-1989 | Chicago | Ambient aeroallergen | The odds of a death caused by asthma occurring on days with mold spore counts of 1000 spores per cubic meter or greater was 2.16 times higher (95% CI = 1.31–3.56, p = 0.003) than on days on which mold spore counts were less than 1000 spores per cubic meter. |
| Bolte et al. [54] | Cohort | Munich and Leipzig, Germany | Endotoxin | High endotoxin levels increased the risk of repeated wheeze (OR = 1.52; CI = 1.08–2.14). | |
| Loh et al. [57] | Cross-sectional | 18 healthy non-atopic human subjects | Inhaled endotoxin or lipopolysaccharide (LPS) | Myeloperoxidase, human neutrophil elastase and interleukin-8 in sputum sol, showed a trend towards greater increase following 50 μg LPS. | |
| Alexis et al. [61] | Toxicological | 9 Healthy subjects | Chapel Hill, NC | PM2.5–10, biologic material on PM2.5–10 | Induced elevated inflammation; increased eotaxin, and increased phagocytosis. |
| Cakmak et al. [80] | Cross-sectional | Children presented with diagnosed conjunctivitis or rhinitis 1993–1997 | Eastern Ontario, Canada | Fungal spores and pollen grains | An increase of 551 basidiomycete’s spores per m3, or of 72 ragweed grains per m3, was associated with an increase of about 10% in hospital visits for conjunctivitis and rhinitis. |
| Adhikari et al. [81] | Cross-sectional | Adult showing symptoms of type-I respiratory allergy | India | Airborne viable and non-viable fungi | 52% of the viable airborne fungi identified were allergenic. |
| Study | Type of Study | Study Population | Study Location | Component Analyzed | Health Outcome |
|---|---|---|---|---|---|
| Jacobs et al. [17] | Cross-sectional | 88 non-smoking individuals | Antwerp, Belgium | PM2.5, PAHs, transition metals | Increase of 20.8 μg/m³ in 24-h mean outdoor PM2.5 was associated with an increase in pulse pressure of 4.0 mmHg (95% CI = 1.8–6.2); V, Fe and Ni contents of PM2.5 were significantly associated with systolic blood pressure and pulse pressure; chrysene-5, 6-dione and benzo(a)pyrene-3,6-dione were significantly associated with increases in systolic blood pressure and pulse pressure. |
| Osornio-Vargas et al. [63] | Toxicological | N/A | N/A | EC, bacteria on PMs | PM2.5 and PM10 samples caused cytotoxicity; PM2.5 induces cytotoxicity in vitro through an endotoxin-independent mechanism that is likely mediated by transition metals; PM10 with relatively high levels of endotoxin induces proinflammatory cytokine release via an endotoxin-dependent mechanism. |
| Bell et al. [89] | Cross-sectional | General population >64 years 1999–2005 | 106 U.S. Counties | PM2.5, Vanadium, nickel, elemental carbon | Positive association between county-specific estimates of short-term effects of PM2.5 on cardiovascular and respiratory hospitalizations and county-specific levels of V, EC, or Ni PM2.5 content. |
| Peng et al. [90] | Cross-sectional | General population 2000–2006 | 119 U.S urban communities | PM2.5, sulfate, nitrate, Si, elemental carbon, organic carbon matter, sodium, ammonium ions | Ambient levels of elemental carbon and organic carbon matter are associated with risks of emergency hospitalization. |
| Ostro et al. [91] | Cross-sectional | General population | Six California counties | PM2.5 mass and components, including elemental and organic carbon (EC and OC), nitrates, sulfates, and various metal | PM2.5 mass and several constituents were associated with multiple mortality categories, especially cardiovascular death. |
| Zanobetti et al. [92] | Cross-sectional | General population 2000–2003 | US communities | PM2.5, elemental composition, ionic species | For a 10 μg/m3 increase in 2-day averaged PM2.5 concentration, there was an increase of 1.89% in CVD, 2.74% (95% CI: 1.30–4.2) in diabetes, and 2.07% (95% CI: 1.20–2.95) in respiratory admissions; PM2.5 mass was higher in Ni, As, and Cr, as well as Br and OC significantly increased its effect on hospital admissions. |
| Bell et al. [94] | Cross-sectional | 3 Connecticut counties and 1 Massachusetts county | PM2.5, 50 elements, traffic, road dust/crustal | Increase in exposure was associated with low birthweight for Zn, EC, Si, Al, V, and Ni. Analysis by trimester showed effects of third-trimester exposure to EC, Ni, V, and oil combustion PM2.5. | |
| Diaz and Dominguez [101] | Cross-sectional | General population | Mexico | EC of PM2.5 | High risk of contracting diseases associated with elemental exposure. |
| Gavett and Koren [102] | Toxicological | Healthy volunteers | NA | Ambient PM, Transition metals | Formation of reactive oxygen species and subsequent lung injury, inflammation, and airway hyper responsiveness leading to airflow limitation and symptoms of asthma. |
| Boffetta et al. [103] | Cross-sectional | Industrial workers | PAHs and nitro-PAHs | Risk of lung, skin, and bladder cancer. | |
| Perera et al. [104] | Cross-sectional | 867 mothers and 822 newborns | Northern Manhattan, The World Trade Center Area, Poland, and China | PM, PAH, benzo( a)pyrene | Fetus may be 10-fold more susceptible to DNA damage than the mother and that in utero exposure to PAH may disproportionately increase carcinogenic risk. |
| Edwards et al. [105] | Cohort study | Pregnant, healthy, non-smoking women | Krakow, Poland | PAH | Prenatal exposure to PAH was associated with decreased Raven Colored Progressive Matrices (RCPM) scores at age 5. |
| Pope et al. [106] | Cross-sectional | General population 1980–1989 | U.S. | PM, Sulfate | PM was associated with cardiopulmonary and lung cancer mortality; Increased mortality is associated with sulfate and PM2.5 at levels commonly found in U.S. cities. |
| Burnett et al. [107] | Cross-sectional | General population 1983–1988 | Ontario, Canada | Sulfate | A 13 μg/m3 increase in sulfates was associated with a 3.7% increase in respiratory admissions and a 2.8% increase in cardiac admissions for all age groups. |
| Delfino et al. [108] | Cross-sectional | Patients with respiratory illnesses 1992–1993 | Montreal, Quebec | PM2.5, PM10, O3, SO42− | 1-h maximum O3, PM10, PM2.5, and SO42− were all positively associated with respiratory visits for patients over 64 yrs. of age. |
| Bennet et al. [109] | Cross-sectional | General population 1997–1999 | Vancouver region of British Columbia, Canada | PM10, Desert Dust | Additional one or two hospitalizations per 100,000 population for respiratory and cardiac illnesses. |
| Bonner et al. [110] | Toxicological study | General population | Mexico city | Endotoxins, elemental contents of PM10 | PM10 induce expression of the PDGF a-receptor subtype on rat pulmonary myofibroblasts; endotoxin and metal components of PM10 stimulate IL-1b release. Endotoxin on PM10 particles elicited upregulation of the PDGF receptor. |
| Dockery et al. [111] | Cross-sectional | ICD Patients | Boston | PM2.5, BC, sulfate | Ventricular tachyarrhythmias. |
| Frampton et al. [112] | Cross-sectional | General population | Utah valley | Metal content of PM10 | Cytotoxicity, induced expression of interleukin-6 and -8. |
| Ghio et al. [113] | Toxicological | 38 Healthy volunteers | North Carolina | Ambient particles | Mild inflammation in the lower respiratory tract, and increased concentration of blood fibrinogen. |
| Hsu et al. [114] | Cross-sectional | Elderly patients | New York City | PM2.5, PM10, , Elemental carbon (EC), K, Ni, Ca, Fe, Al, Si, Se, V, Zn | Cardiopulmonary function parameters. |
| Lall et al. [115] | Cross-sectional | Medicare hospital Admissions | New York City | EC, Ni, Mn, Si, S | Daily hospital admissions, 2001–2002. |
| Strickland et al. [116] | Cross-sectional | Children 5–17 Years 1993–2004 | Atlanta | PM10, PM2.5, sulfate, EC, OC, water-soluble Metals | Emergency department visits for asthma. |
| Thurston et al. [117] | Cross-sectional | General population 1986–1988 | Toronto, Ontario | PM2.5, PM10, O3, (H+) and sulfates (SO4−) | Exposure to O3, H+, and SO4− were significantly associated with respiratory and asthma admissions. |
| Wellenius et al. [118] | Cross-sectional | Hospitalized stroke Patients 1999–2008 | Boston area | PM2.5, BC, sulfate | Stroke onset. |
| Zhou et al. [119] | Cross-sectional | General population | Detroit, Seattle | PM2.5, Al, Fe, K, Na, Ni, S, Si, V, Zn, EC | Mortality: total, cardiovascular, respiratory. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morakinyo, O.M.; Mokgobu, M.I.; Mukhola, M.S.; Hunter, R.P. Health Outcomes of Exposure to Biological and Chemical Components of Inhalable and Respirable Particulate Matter. Int. J. Environ. Res. Public Health 2016, 13, 592. https://doi.org/10.3390/ijerph13060592
Morakinyo OM, Mokgobu MI, Mukhola MS, Hunter RP. Health Outcomes of Exposure to Biological and Chemical Components of Inhalable and Respirable Particulate Matter. International Journal of Environmental Research and Public Health. 2016; 13(6):592. https://doi.org/10.3390/ijerph13060592
Chicago/Turabian StyleMorakinyo, Oyewale Mayowa, Matlou Ingrid Mokgobu, Murembiwa Stanley Mukhola, and Raymond Paul Hunter. 2016. "Health Outcomes of Exposure to Biological and Chemical Components of Inhalable and Respirable Particulate Matter" International Journal of Environmental Research and Public Health 13, no. 6: 592. https://doi.org/10.3390/ijerph13060592