Point-of-Care Diagnostic Tests for Detecting SARS-CoV-2 Antibodies: A Systematic Review and Meta-Analysis of Real-World Data

 ,
,  , and
, and
Abstract
:1. Introduction
2. Experimental Section
- (1)
- Settings of the study;
- (2)
- Characteristics of reference cases;
- (3)
- Characteristics of reference diagnostic test;
- (4)
- Characteristics of the commercially available point-of-care test employed; and,
- (5)
- Total number of true positive, true negative, false positive, false negative cases.
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A


Appendix B

References
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.; Chen, R.; Tang, C.; Wang, T.; et al. Comorbidity and Its Impact on 1590 Patients with Covid-19 in China: A Nationwide Analysis. Eur. Respir. J. 2020, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Diseases Prevention and Control (ECDC). An Overview of the Rapid Test Situation for COVID-19 Diagnosis in the EU/EEA. Stockholm. 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Overview-rapid-test-situation-for-COVID-19-diagnosis-EU-EEA.pdf (accessed on 29 April 2020).
- Tang, Y.-W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. The Laboratory Diagnosis of COVID-19 Infection: Current Issues and Challenges. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vashist, S.K. In Vitro Diagnostic Assays for COVID-19: Recent Advances and Emerging Trends. Diagnostics 2020, 10, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassaniti, I.; Novazzi, F.; Giardina, F.; Salivaro, F.; Sachs, M.; Perlini, S.; Bruno, R.; Mojoli, F.; Baldanti, F. San Matteo Pavia COVID-19 Task Force. Performance of VivaDiagTM COVID-19 IgM/IgG Rapid Test Is Inadequate for Diagnosis of COVID-19 in Acute Patients Referring to Emergency Room Department. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Lassaunière, R.; Frische, A.; Harboe, Z.B.; Nielsen, A.C.Y.; Fomsgaard, A.; Karen, A.; Jørgensen, C.S. Evaluation of Nine Commercial SARS-CoV-2 Immunoassays. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Loeffelholz, M.J.; Tang, Y.-W. Laboratory Diagnosis of Emerging Human Coronavirus Infections—The State of the Art. Emerg. Microbes Infect. 2020, 9, 747–756. [Google Scholar] [CrossRef]
- Virgilio Paradiso, A.; De Summa, S.; Loconsole, D.; Procacci, V.; Sallustio, A.; Centrone, F.; Silvestris, N.; Cafagna, V.; De Palma, G.; Tufaro, A.; et al. Clinical meanings of rapid serological assay in patients tested for SARS-Co2 RT-PCR. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Garcia, F.; Pérez-Tanoira, R.; Romanyk, J.; Arroyo, T.; Gómez-Herruz, P.; Cuadros-González, J. Rapid Diagnosis of SARS-CoV-2 Infection by Detecting IgG and IgM Antibodies with an Immunochromatographic Device: A Prospective Single-Center Study. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Diao, B.; Wen, K.; Chen, J.; Liu, Y.; Yuan, Z.; Han, C.; Chen, J.; Pan, Y.; Chen, L.; Dan, Y.; et al. Diagnosis of Acute Respiratory Syndrome Coronavirus 2 Infection by Detection of Nucleocapsid Protein Running Title: Diagnosis of COVID-19 by N Antigen Detection. medRxiv 2020. [Google Scholar] [CrossRef]
- Harrington, A.; Cox, B.; Snowdon, J.; Bakst, J.; Ley, E.; Grajales, P.; Maggiore, J.; Kahn, S. Comparison of Abbott ID Now and Abbott M2000 Methods for the Detection of SARS-CoV-2 from Nasopharyngeal and Nasal Swabs from Symptomatic Patients. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Odiwuor, N.; Xiong, J.; Sun, L.; Nyaruaba, R.O.; Wei, H.; Tanner, N.A.; Tanner, N. Rapid Molecular Detection of SARS-CoV-2 (COVID-19) Virus RNA Using Colorimetric LAMP. medRxiv 2020. [Google Scholar] [CrossRef]
- González-González, E.; Trujillo-de Santiago, G.; Montserrat Lara-, I.; Omar Martínez-Chapa, S.; Moisés Alvarez, M.; León, N. Portable and Accurate Diagnostics for COVID-19: 1 Combined Use of the MiniPCR® Thermocycler and a Well-Plate Reader for SARS-CoV-2 Virus Detection. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Riccò, M.; Ferraro, P.; Gualerzi, G.; Ranzieri, S.; Bragazzi, N.L.; Balzarini, F.; Signorelli, C. Point-of-Care Diagnostic of SARS-CoV-2: Knowledge, Attitudes, and Beliefs (KAP) of Medical Workforce in Italy. Acta Biomed. 2020, 91. [Google Scholar] [CrossRef]
- Long, Q.; Liu, B.; Deng, H.; Wu, G.; Deng, K.; Chen, Y.; Liao, P.; Qiu, J.; Lin, Y.; Cai, X.; et al. Antibody Responses to SARS-CoV-2 in Patients with COVID-19. Nat. Med. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Advice on the Use of Point-of- Care Immunodiagnostic Tests for COVID-19. Available online: https://www.who.int/news-room/commentaries/detail/advice-on-the-use-of-point-of-care-immunodiagnostic-tests-for-covid-19 (accessed on 28 April 2020).
- Mutti, A. Occupational Medicine in the Time of COVID-19/La Medicina Del Lavoro Ai Tempi Del COVID-19. Medicina del lavoro 2020, 111, 83–86. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Bizzaro, N.; Villalta, D.; Giavarina, D.; Tozzoli, R. Are Anti-Nucleosome Antibodies a Better Diagnostic Marker than Anti-DsDNA Antibodies for Systemic Lupus Erythematosus? A Systematic Review and a Study of Metanalysis. Autoimmun. Rev. 2012, 12, 97–106. [Google Scholar] [CrossRef]
- Döhla, M.; Boesecke, C.; Schulte, B.; Diegmann, C.; Sib, E.; Richter, E.; Eschbach-Bludau, M.; Aldabbagh, S.; Marx, B.; Eis-Hübinger, A.-M.; et al. Rapid Point-of-Care Testing for SARS-CoV-2 in a Community Screening Setting Shows Low Sensitivity. Public Health 2020, 182, 170–172. [Google Scholar] [CrossRef]
- Adams, E.; Ainsworth, M.; Anand, R.; Andersson, M.; Auckland, K.; Baillie, K.; Barners, E.; Beer, S.; Bell, J.; Berry, T.; et al. Evaluation of Antibody Testing for SARS-CoV-2 Using ELISA and Lateral Flow Immunoassays. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Ling, E.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; et al. COVID-19 Antibody Seroprevalence in Santa Clara County, California. medRxiv 2020. [Google Scholar] [CrossRef]
- Xiang, J.; Yan, M.; Li, H.; Liu, T.; Lin, C.; Huang, S.; Shen, C. Evaluation of Enzyme-Linked Immunoassay and Colloidal Gold- Immunochromatographic Assay Kit for Detection of Novel Coronavirus (SARS-Cov-2) Causing an Outbreak of Pneumonia (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Liu, Y.; Diao, B.; Ren, F.; Wang, Y.; Ding, J.; Huang, Q. Diagnostic Indexes of a Rapid IgG/IgM Combined Antibody Test for SARS-CoV-2. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Tabata, S.; Ikeda, M.; Noguchi, S.; Kitagawa, Y.; Matsuoka, M.; Miyoshi, K.; Tarumoto, N.; Sakai, J.; Ito, T.; et al. Clinical Evaluation of an Immunochromatographic IgM/IgG Antibody Assay and Chest Computed Tomography for the Diagnosis of COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W.; et al. Development and Clinical Application of A Rapid IgM-IgG Combined Antibody Test for SARS-CoV-2 Infection Diagnosis. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Lian, J.; Jin, X.; Hao, S.; Cai, H.; Zhang, S.; Zheng, L.; Jia, H.; Hu, J.; Gao, J.; Zhang, Y.; et al. Analysis of Epidemiological and Clinical Features in Older Patients with Corona Virus. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of Comorbidities in the Novel Wuhan Coronavirus (COVID-19) Infection: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Bovo, C.; Plebani, M.; Services, S. Current Laboratory Diagnostics of Coronavirus Disease 2019 (COVID-19). Acta Biomed. 2020. [Google Scholar] [CrossRef]
- Pan, Y.; Li, X.; Yang, G.; Fan, J.; Tang, Y.; Zhao, J.; Long, X.; Guo, S.; Zhao, Z.; Liu, Y.; et al. Serological Immunochromatographic Approach in Diagnosis with SARS-CoV-2 Infected COVID-19 Patients. J. Infect. 2020. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Characteristics of the Samples | Commercial Test | No. of Samples | TP | FP | FN | TN | Se. | Sp. | PPV | PNV | Accuracy | Cohen’s Kappa |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Imai et al. 2020 [27] | 139 samples from 112 COVID-19 patients, 48 negative patients from Saitama Hospital | Artron laboratories | 187 | 60 | 1 | 79 | 47 | 42.2% | 97.9% | 98.4% | 37.3% | 57.2% | 0.268 |
| Lassaunière et al. 2020 [8] | 30 COVID-19 confirmed cases admitted to intensive care unit vs. 10 samples from healthy donors + patients with previous history of coronarivus infection (N = 5), non-coronavirus respiratory infection (N = 45), dengue (N = 9), CMV (N = 2), EBV (N = 10). | Artron Laboratories | 47 | 25 | 0 | 5 | 17 | 83.3% | 100% | 100% | 77.3% | 89.4% | 0.783 |
| Acro Biotech | 20 | 4 | 3 | 1 | 12 | 80.0% | 80.0% | 57.1% | 92.3% | 80.0% | 0.529 | ||
| AutoBio Diagnostics | 62 | 28 | 0 | 2 | 32 | 93.3% | 100% | 100% | 94.1% | 96.8% | 0.935 | ||
| Dynamiker | 62 | 27 | 0 | 3 | 32 | 90.0% | 100% | 100% | 91.4% | 95.2% | 0.903 | ||
| CTK Biotech | 62 | 27 | 0 | 3 | 32 | 90.0% | 100% | 100% | 91.4% | 95.2% | 0.903 | ||
| Cassaniti et al. 2020 [7] | 30 negative healthy controls vs. 30 COVID-19 cases tested with both POCT and RT-PCR | VivaDiag | 60 | 19 | 0 | 11 | 30 | 63.3% | 100% | 100% | 73.2% | 81.7% | 0.633 |
| 50 subjects with suspected COVID-19 sequentially tested with POCT and RT-PCR | VivaDiag | 50 | 7 | 1 | 31 | 11 | 18.4% | 91.7% | 87.5% | 26.2% | 36.0% | 0.054 | |
| Virgilio Paradiso et al. 2020 [10] | 191 cases with suspected COVID-19 sequentially tested with POCT and RT-PCR | VivaDiag | 191 | 21 | 13 | 49 | 107 | 30.0% | 89.2% | 61.8% | 68.6% | 67.4% | 0.215 |
| Perez-Garcia et al. 2020 [11] | 45 healthy controls vs. 55 SARS-CoV-2 cases | AllTest Biotech | 100 | 26 | 0 | 29 | 45 | 47.3% | 100% | 100% | 60.8% | 71.0% | 0.447 |
| Döhla et al. 2020 [22] | 39 cases randomly selected among subjects referring to a German COVID-19 screening center | Undisclosed manufacturer | 49 | 8 | 3 | 14 | 27 | 36.4% | 88.9% | 72.7% | 63.2% | 65.3% | 0.265 |
| Bendavid et al. 2020 [24] | 30 orthopedic patients, samples collected before COVID-19 pandemics; 37 PCR confirmed COVID-19 samples | Premier Biotech | 67 | 25 | 0 | 12 | 30 | 67.6% | 100% | 100% | 71.4% | 82.1% | 0.651 |
| Xiang et al. 2020 [25] | 35 healthy individuals; 91 RT-PCR confirmed plasma samples from COVID-19 patients | Zhuhai Livzon Diagnostics | 126 | 75 | 0 | 16 | 35 | 82.4% | 100% | 100% | 68.6% | 87.3% | 0.723 |
| Adams et al. 2020 [23] | Random samples from a pool of 40 SARS-CoV-2 positive blood samples, and 50 SARS-CoV-2 negative blood samples | Undisclosed manufacturers | 93 | 18 | 0 | 15 | 60 | 54.5% | 100% | 100% | 80.0% | 54.5% | 0.608 |
| 128 | 23 | 1 | 14 | 90 | 62.2% | 98.9% | 95.8% | 86.5% | 62.2% | 0.682 | |||
| 93 | 21 | 2 | 12 | 58 | 63.6% | 96.7% | 91.3% | 82.0% | 63.6% | 0.647 | |||
| 98 | 25 | 1 | 13 | 59 | 65.8% | 98.3% | 96.2% | 81.9% | 65.8% | 0.681 | |||
| 91 | 19 | 2 | 12 | 58 | 61.3% | 96.7% | 90.5% | 82.9% | 61.3% | 0.629 | |||
| 91 | 20 | 1 | 11 | 59 | 64.5% | 98.3% | 95.2% | 84.3% | 64.5% | 0.682 | |||
| 93 | 23 | 3 | 10 | 57 | 69.7% | 95.0% | 88.5% | 85.1% | 69.7% | 0.679 | |||
| 92 | 18 | 0 | 14 | 60 | 56.3% | 100% | 100% | 81.1% | 56.3% | 0.626 | |||
| 212 | 22 | 4 | 48 | 138 | 31.4% | 97.2% | 84.6% | 74.2% | 31.4% | 0.340 | |||
| Liu et al. 2020 [26] | 179 consecutive patients, grouped by results of RT-PCR in SARS-CoV-2 positive (No.90), and negative ones (No.89) | Undisclosed manufacturer | 179 | 77 | 13 | 8 | 81 | 90.6% | 86.2% | 85.6% | 91.0% | 88.3% | 0.765 |
| Property | Value | 95%CI |
|---|---|---|
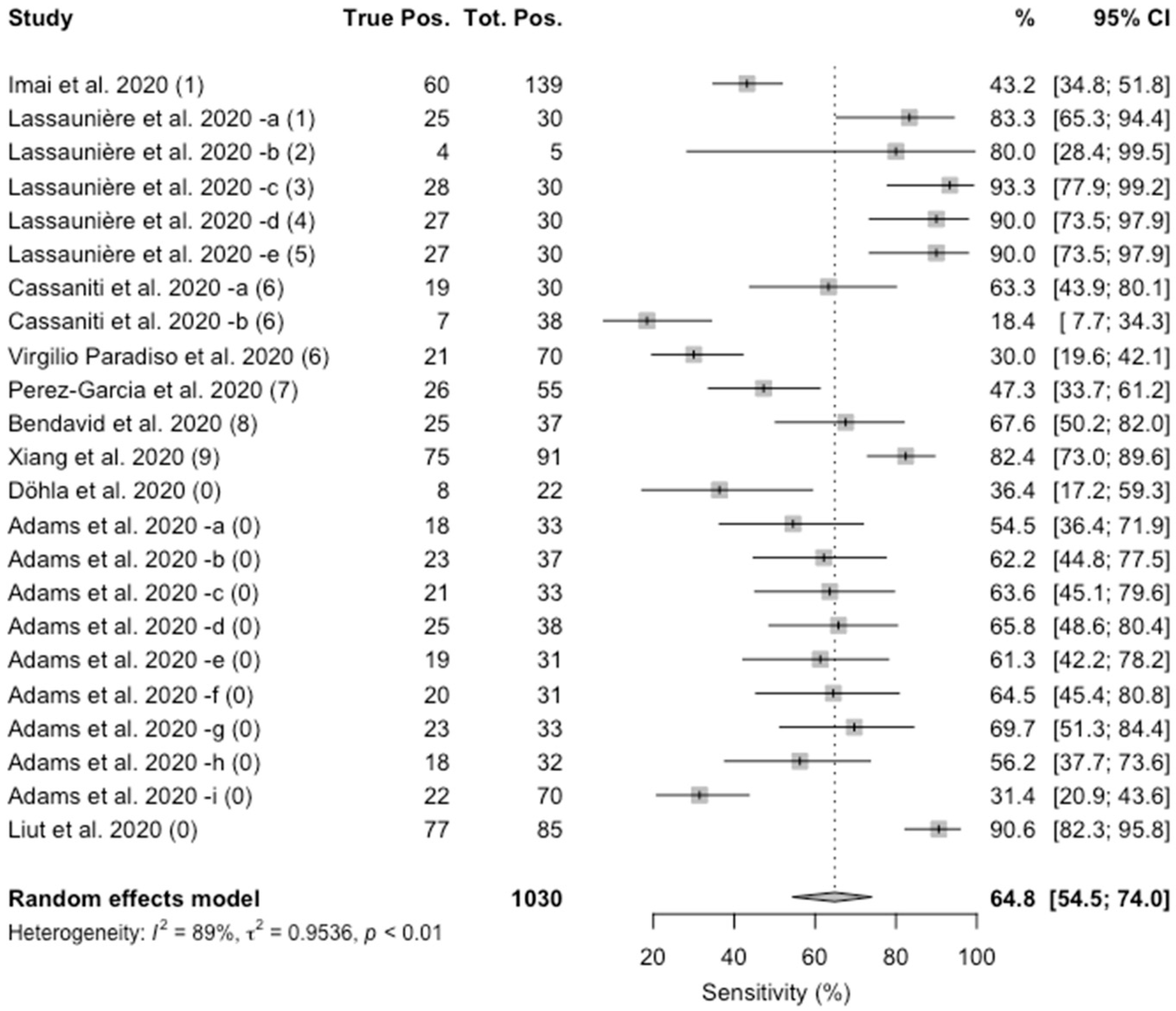
| Sensitivity (%) | 64.8 | 54.5; 74.0 |
| Specificity (%) | 98.0 | 95.8; 99.0 |
| PLR | 14.2 | 8.7; 23.2 |
| NLR | 0.4 | 0.2; 0.5 |
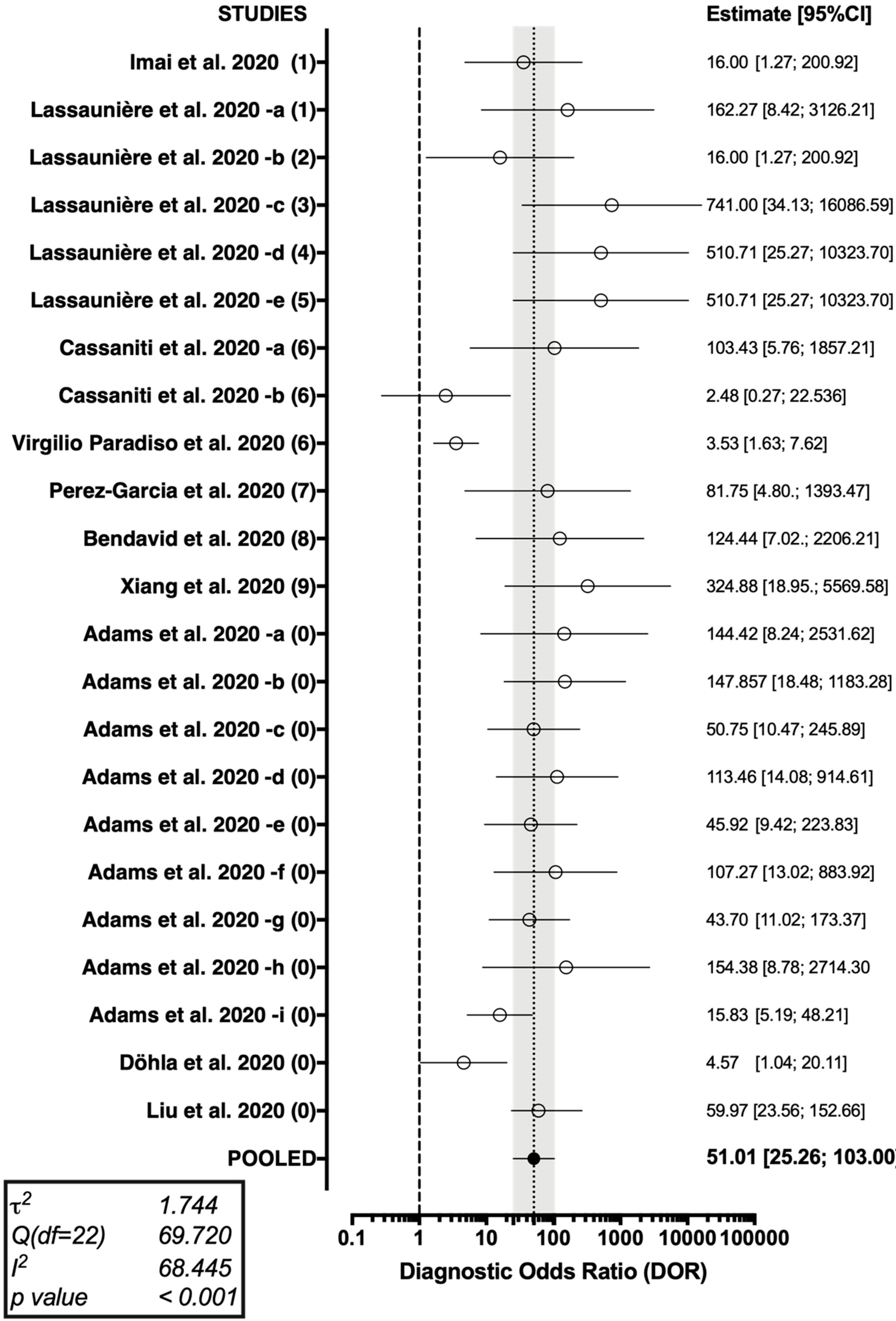
| DOR | 51.01 | 25.26; 103.00 |
| Cohen’s kappa | 0.594 | 0.496; 0.691 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Ferraro, P.; Gualerzi, G.; Ranzieri, S.; Henry, B.M.; Said, Y.B.; Pyatigorskaya, N.V.; Nevolina, E.; Wu, J.; Bragazzi, N.L.; et al. Point-of-Care Diagnostic Tests for Detecting SARS-CoV-2 Antibodies: A Systematic Review and Meta-Analysis of Real-World Data. J. Clin. Med. 2020, 9, 1515. https://doi.org/10.3390/jcm9051515
Riccò M, Ferraro P, Gualerzi G, Ranzieri S, Henry BM, Said YB, Pyatigorskaya NV, Nevolina E, Wu J, Bragazzi NL, et al. Point-of-Care Diagnostic Tests for Detecting SARS-CoV-2 Antibodies: A Systematic Review and Meta-Analysis of Real-World Data. Journal of Clinical Medicine. 2020; 9(5):1515. https://doi.org/10.3390/jcm9051515
Chicago/Turabian StyleRiccò, Matteo, Pietro Ferraro, Giovanni Gualerzi, Silvia Ranzieri, Brandon Michael Henry, Younes Ben Said, Natalia Valeryevna Pyatigorskaya, Elena Nevolina, Jianhong Wu, Nicola Luigi Bragazzi, and et al. 2020. "Point-of-Care Diagnostic Tests for Detecting SARS-CoV-2 Antibodies: A Systematic Review and Meta-Analysis of Real-World Data" Journal of Clinical Medicine 9, no. 5: 1515. https://doi.org/10.3390/jcm9051515