Advances in Degradable Embolic Microspheres: A State of the Art Review

Abstract
:
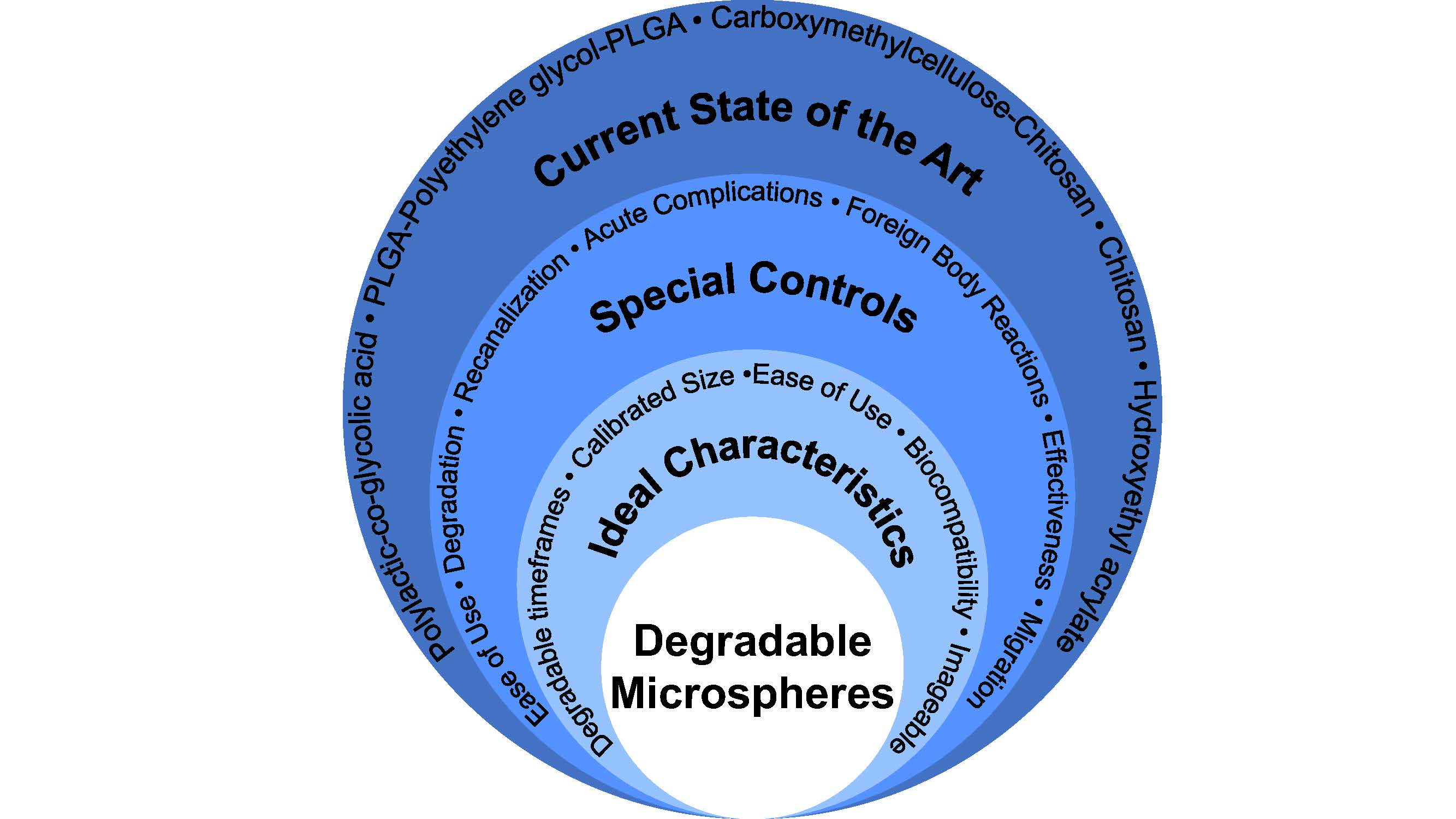
1. Introduction
- Tailored degradation timeframes—to provide adequate infarction to the target tissues in a variety of indications, subsequently allowing return of flow (e.g., 5–7 h for uterine artery embolization—based on Doppler-guided transvaginal clamping) [2]
- A variety of tightly calibrated particle size distributions—to optimize particle delivery according to target artery anatomy [3]
- Ease of delivery through conventional microcatheters—to facilitate adoption of the novel technology into established embolization techniques
- Full biological compatibility as per the relevant sections of ISO-10993—to minimize safety concerns [4]
- Multi-modal imageability (e.g., fluoroscopy, CT)—to allow for efficiency and standardization of embolization endpoints [5].
2. Methodology
3. Current State of the Art
3.1. PLGA
3.1.1. PLGA: Basic Chemistry and Mechanisms of Degradation
3.1.2. PLGA: Safety, Efficacy and Performance
3.1.3. Key Advantages of PLGA Microspheres (Occlusin® 500 Artificial Embolization Device)
- Approved by FDA for the treatment of unresectable/inoperable hypervascularized tumors (k093813) [23]
- Available in multiple particle size ranges for a variety of applications
- Easily suspended in conventional contrast media and delivered using standard embolization equipment
- Demonstrated full biological compatibility (via testing performed to obtain device clearance)
- Mitigate the risk of migration through biological occlusion (fibrous ingrowth anchoring the particles in place as they degrade).
3.1.4. Key Limitations of PLGA Microspheres (Occlusin® 500 Artificial Embolization Device)
- Lack of tailorable degradation timeframes—6 to 12 months occlusion timeframe only
- Lacks multi-modal imageability.
3.2. PLGA-PEG-PLGA
3.2.1. PLGA-PEG-PLGA: Basic Chemistry and Mechanisms of Degradation
3.2.2. PLGA-PEG-PLGA: Safety, Efficacy and Performance
3.2.3. Key Advantages of PLGA-PEG-PLGA Microspheres
- Limit necrotic damage due to rapid degradation timeframe (ca. <24 h)
- Available in multiple particle size ranges for a variety of applications
- Comparable ease of delivery to control article.
3.2.4. Key Limitations of PLGA-PEG-PLGA Microspheres
- Lack of tailorable degradation timeframes—ca. seven-day timeframe only
- Toxicity concerns related to PEG degradation byproducts not directly addressed, may not offer full biological compatibility
- Lacks multi-modal imageability.
3.3. CMC-CNN
3.3.1. CMC-CNN: Basic Chemistry and Mechanisms of Degradation
3.3.2. CMC-CNN: Safety, Efficacy and Performance
3.3.3. Key Advantages of CMC-CNN Microspheres
- Potentially offers a range of tailorable degradation timeframes based on in vitro evaluations
- Available in a wide variety of particle sizes from 100 to 1550 µm
- Superior ease of delivery as compared to the control (less adhesive) using conventional embolization equipment.
3.3.4. Key Limitations of CMC-CNN Microspheres
- No information on in vivo degradation timeframes or recanalization
- Toxicity concerns related to degradation byproducts and their size(s) not addressed, may not offer full biological compatibility
- Lacks multi-modal imageability.
3.4. Chitosan
3.4.1. Chitosan: Basic Chemistry and Mechanisms of Degradation
3.4.2. Chitosan: Safety, Efficacy and Performance
3.4.3. Key Advantages of Chitosan Microspheres
- Easily delivered through conventional microcatheters and provides for more compact vessel occlusion (relative to irregular PVA particles)
- Low risk of local and systemic toxicity (unlikely a high-risk allergen)—potential to fulfill full biological compatibility
- Extended degradation timeframe potentially mitigates risk of migration through stimulation of fibrous ingrowth.
3.4.4. Key Limitations of Chitosan Microspheres
- No information provided on ability to manufacture different particle size ranges
- Lack of tailorable degradation timeframes—24 to 34 week occlusion timeframe only
- Lacks multi-modal imageability.
3.5. HEA
3.5.1. HEA: Basic Chemistry and Mechanisms of Degradation
3.5.2. HEA: Safety, Efficacy and Performance
3.5.3. Key Advantages of HEA Microspheres
- Produced notably lower levels of ischemia relative to control agent
3.5.4. Key Limitations of HEA Microspheres
- No information provided on ability to manufacture different particle size ranges
- No information provided on ease of use of microspheres
- Lack of tailorable degradation timeframes—2 to 3 week occlusion timeframe only
- Toxicity of degradation byproducts (e.g., putrescine) not assessed
- Lacks multi-modal imageability.
4. Preclinical Models
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Forster, R.E.J.; Thürmer, F.; Wallrapp, C.; Lloyd, A.W.; Macfarlane, W.; Phillips, G.J.; Boutrand, J.-P.; Lewis, A.L. Characterisation of physico-mechanical properties and degradation potential of calcium alginate beads for use in embolisation. J. Mater. Sci. 2010, 21, 2243–2251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verret, V.; Pelage, J.P.; Wassef, M.; Louguet, S.; Servais, E.; Bédouet, L.; Beaulieu, T.; Moine, L.; Laurent, A. A novel resorbable embolization microsphere for transient uterine artery occlusion: A comparative study with trisacryl-gelatin microspheres in the Sheep Model. JVIR 2014, 25, 1759–1766. [Google Scholar] [CrossRef] [PubMed]
- Kessel, D.; Ray, C. Transcatheter embolization and therapy. In Techniques in Interventional Radiology, 1st ed.; Springer: London, UK, 2010. [Google Scholar]
- Food and Drug Administration Center for Devices and Radiological Health. Guidance for Industry and FDA Staff: Class II Special Controls Guidance Document: Vascular and Neurovascular Embolization Devices; Food and Drug Administration Center for Devices and Radiological Health: Silver Spring, MD, USA, 2004.
- Kehoe, S.; Amensag, S.; Looney, M.; Abraham, R.J.; Boyd, D. “Imageable” zinc-silicate glass microspheres for transarterial embolization: A renal artery embolization study. Biomed. Glasses 2015, 1. [Google Scholar] [CrossRef]
- Bohner, M. Resorbable biomaterials as bone graft substitutes. Mater. Today 2010, 13, 24–30. [Google Scholar] [CrossRef]
- Williams, D. Essential Biomaterials Science; Cambridge University Press: Cambridge, UK, 2014; ISBN 978-0-521-89908-6. [Google Scholar]
- Gupta, B.; Revagade, N.; Hilborn, J. Poly(lactic acid) fiber: An overview. Progress Polym. Sci. 2007, 32, 455–482. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An overview of Poly(lactic-co-glycolic) acid (PLGA)-based biomaterials for bone tissue engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-co-Glycolic ACID (PLGA) as biodegradable controlled drug delivery carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef] [PubMed]
- You, Y.; Lee, S.W.; Youk, J.H.; Min, B.-M.; Lee, S.J.; Park, W.H. In vitro degradation behaviour of non-porous ultra-fine poly(glycolic acid)/poly(l-lactic acid) fibres and porous ultra-fine poly(glycolic acid) fibres. Polym. Degrad. Stab. 2005, 90, 441–448. [Google Scholar] [CrossRef]
- Houchin, M.L.; Topp, E.M. Chemical degradation of peptides and proteins in PLGA: A review of reactions and mechanisms. J. Pharm. Sci. 2008, 97, 2395–2404. [Google Scholar] [CrossRef] [PubMed]
- Grayson, A.C.R.; Voskerician, G.; Lynn, A.; Anderson, J.M.; Cima, M.J.; Langer, R. Differential degradation rates in vivo and in vitro of biocompatible poly(lactic acid) and poly(glycolic acid) homo- and co-polymers for a polymeric drug-delivery microchip. J. Biomater. Sci. 2004, 15, 1281–1304. [Google Scholar] [CrossRef]
- Xu, Y.; Kim, C.-S.; Saylor, D.M.; Koo, D. Polymer degradation and drug delivery in PLGA-based drug–polymer applications: A review of experiments and theories. J. Biomed. Mater. Res. 2017, 105, 1692–1716. [Google Scholar] [CrossRef] [PubMed]
- Rasal, R.M.; Janorkar, A.V.; Hirt, D.E. Poly(lactic acid) modifications. Progress Polym. Sci. 2010, 35, 338–356. [Google Scholar] [CrossRef]
- Boland, E.L.; Shine, R.; Kelly, N.; Sweeney, C.A.; McHugh, P.E. A review of material degradation modelling for the analysis and design of bioabsorbable stents. Ann. Biomed. Eng. 2016, 44, 341–356. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, S.; Reddy, B.S.R. Bio-absorbable polymers in implantation—An overview. JSIR 2009, 68, 993–1009. [Google Scholar]
- Owen, R.J.; Nation, P.N.; Polakowski, R.; Biliske, J.A.; Tiege, P.B.; Griffith, I.J. A preclinical study of the safety and efficacy of OcclusinTM 500 artificial embolization device in Sheep. CardioVasc. Interv. Radiol. 2012, 35, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Revised 501(k) Summary for IMBiotechnologies Ltd. Occlusin 500 Artificial Embolization Device (Per 21CFR 807.92). 2010. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf9/K093813.pdf (accessed on 20 June 2017).
- Stuart, S.; Mayo, J.R.; Ling, A.; Schulzer, M.; Klass, D.; Power, M.A.; Roberton, B.J.; Wan, J.M.; Liu, D.M. Retrospective study of the impact of fellowship training on two quality and safety measures in uterine artery embolization. J. Am. Coll. Radiol. 2014, 11, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Vilos, G.A.; Vilos, E.C.; Romano, W.; Abu-Rafea, B. Temporary uterine artery occlusion for treatment of menorrhagia and uterine fibroids using an incisionless Doppler-guided transvaginal clamp: Case report. Hum. Reprod. 2006, 21, 269–271. [Google Scholar] [CrossRef] [PubMed]
- “Use of International Standard ISO-10993, Biological Evaluation of Medical Devices Part 1: Evaluation and Testing” PDF. Available online: https://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm348890.pdf (accessed on 11 July 2017).
- Merit Medical Systems, Inc. Embosphere Microspheres Brochure. Available online: https://www.merit.com/interventional-oncology-spine/embolotherapy/microspheres/embosphere-microspheres/#tab-id-2 (accessed on 11 July 2017).
- Swielim, G.E.A. ATLAS—Anatomy of Sheep; Ktab INC.: Cairo, Egypt, 2006; ISBN 978-977-281-292-9. [Google Scholar]
- Webster, R.; Elliott, V.; Park, B.K.; Walker, D.; Hankin, M.; Taupin, P. PEG and PEG conjugates toxicity: Towards an understanding of the toxicity of PEG and its relevance to PEGylated biologicals. In PEGylates Protein Drugs: Basic Science and Clinical Applications; Veronese, F.M., Ed.; Birkhauser Verlag: Basel, Switzerland, 2009; pp. 127–146. [Google Scholar] [CrossRef]
- Magnon, L.; Laurent, A.; Wassef, M.; Bedouet, L.; Louguet, S.; Verret, V.; Servais, E. Implantable Swellable Bio-Resorbable Polymer. Patent 2012/120138, 13 September 2012. [Google Scholar]
- Maeda, N.; Verret, V.; Moine, L.; Bédouet, L.; Louguet, S.; Servais, E.; Osuga, K.; Tomiyama, N.; Wassef, M.; Laurent, A. Targeting and recanalization after embolization with calibrated resorbable microspheres versus hand-cut gelatin sponge particles in a porcine kidney model. J. Vasc. Interv. Radiol. 2013, 24, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- ASTM E11-17. Standard Specification for Woven Wire Test Sieve Cloth and Test Sieves; ASTM International: West Conshohocken, PA, USA, 2017; Available online: https://www.astm.org/Standards/E11.htm (accessed on 20 June 2017).
- Ong, J.L.; Appleford, M.R.; Mani, G. Introduction to Biomaterials: Basic Theory with Engineering Applications; Cambridge University Press: Cambridge, UK, 2013; ISBN 978-0-521-11690-9. [Google Scholar]
- Haraldsson, B.; Nyström, J.; Deen, W.M. Properties of the glomerular barrier and mechanisms of proteinuria. Physiol. Rev. 2008, 88, 451–487. [Google Scholar] [CrossRef] [PubMed]
- Nanosoft Polymers. PLGA-PEG-PLGA. 2015. Available online: https://www.nanosoftpolymers.com/product/plga-peg-plga/ (accessed on 20 June 2017).
- Rosca, C.; Popa, M.I.; Lisa, G.; Chitanu, G.C. Interaction of chitosan with natural or synthetic anionic polyelectrolytes. 1. The chitosan–carboxymethylcellulose complex. Carbohydr. Polym. 2005, 62, 35–41. [Google Scholar] [CrossRef]
- Weng, L.; Le, H.C.; Talaie, R.; Golzarian, J. Bioresorbable Hydrogel Microspheres for Transcatheter Embolization: Preparation and in Vitro Evaluation. J. Vasc. Interv. Radiol. 2011, 22, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, A.; Shrivastava, J. In vitro enzymatic degradation kinetics of polymeric blends of crosslinked starch and carboxymethyl cellulose. Polym. Int. 2005, 54, 1524–1536. [Google Scholar] [CrossRef]
- Reeves, R.; Ribeiro, A.; Lombardo, L.; Boyer, R.; Leach, J.B. Synthesis and characterization of carboxymethylcellulose-methacrylate hydrogel cell scaffolds. Polymers 2010, 2, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Bang, S.; Kim, S.; Jo, S.Y.; Kim, B.-C.; Hwang, Y.; Noh, I. Synthesis and in vitro characterizations of porous carboxymethyl cellulose-poly(ethylene oxide) hydrogel film. Biomater. Res. 2015, 19, 12. [Google Scholar] [CrossRef] [PubMed]
- Kean, T.; Thanou, M. Biodegradation, biodistribution and toxicity of chitosan. Adv. Drug Deliv. Rev. 2010, 62, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Neau, S.H. In vitro degradation of chitosan by bacterial enzymes from rat cecal and colonic contents. Biomaterials 2002, 23, 2761–2766. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Z.; Zhang, J.; Chen, C.; Wu, Q.; Zhang, L.; Zhang, X. Quantitative determination of chitinolytic activity of lysozyme using half-deacetylated chitosan as a substrate. Carbohydr. Polym. 2011, 85, 554–559. [Google Scholar] [CrossRef]
- Yang, Y.M.; Hu, W.; Wang, X.D.; Gu, X.S. The controlling biodegradation of chitosan fibers by N-acetylation in vitro and in vivo. J. Mater. Sci. 2007, 18, 2117–2121. [Google Scholar] [CrossRef] [PubMed]
- Weng, L.; Rusten, M.; Talaie, R.; Hairani, M.; Rosener, N.K.; Golzarian, J. Calibrated bioresorbable microspheres: A preliminary study on the level of occlusion and arterial distribution in a rabbit kidney model. J. Vasc. Interv. Radiol. 2013, 24, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Weng, L.; Rostamzadeh, P.; Nooryshokry, N.; Le, H.C.; Golzarian, J. In vitro and in vivo evaluation of biodegradable embolic microspheres with tunable anticancer drug release. Acta Biomater. 2013, 9, 6823–6833. [Google Scholar] [CrossRef] [PubMed]
- Weng, L.; Seelig, D.; Rostamzadeh, P.; Golzarian, J. Calibrated bioresorbable microspheres as an embolic agent: An experimental study in a rabbit renal model. J. Vasc. Interv. Radiol. 2015, 26, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Pillai, C.K.S.; Paul, W.; Sharma, C.P. Chitin and chitosan polymers: Chemistry, solubility and fiber formation. Progress Polym. Sci. 2009, 34, 641–678. [Google Scholar] [CrossRef]
- Usman, A.; Zia, K.M.; Zuber, M.; Tabasum, S.; Rehman, S.; Zia, F. Chitin and chitosan based polyurethanes: A review of recent advances and prospective biomedical applications. Int. J. Biol. Macromol. 2016, 86, 630–645. [Google Scholar] [CrossRef] [PubMed]
- Kwak, B.K.; Shim, H.J.; Han, S.-M.; Park, E.S. Chitin-based embolic materials in the renal artery of rabbits: Pathologic evaluation of an absorbable particulate agent. Radiology 2005, 236, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Zhang, H.; Metcalfe, A.; Salazkin, I.; Raymond, J. Transcatheter embolization using degradable crosslinked hydrogels. Biomaterials 2004, 25, 5209–5215. [Google Scholar] [CrossRef] [PubMed]
- Ohta, S.; Nitta, N.; Takahashi, M.; Murata, K.; Tabata, Y. Degradable gelatin microspheres as an embolic agent: An experimental study in a rabbit renal model. Korean J. Radiol. 2007, 8, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Jänne, J.; Alhonen, L.; Pietilä, M.; Keinänen, T.A. Genetic approaches to the cellular functions of polyamines in mammals. Eur. J. Biochem. 2004, 271, 877–894. [Google Scholar] [CrossRef] [PubMed]
- Conn, M.P.; Parker, J. The Animal Research War; Palgrave MacMillan US: New York, NY, USA, 2008; ISBN 978-0-230-61199-3. [Google Scholar]
- Davidson, M.K.; Lindsey, J.R.; Davis, J.K. Requirements and selection of an animal model. Isr. J. Med. Sci. 1987, 23, 551–555. [Google Scholar] [PubMed]
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41st ed.; Elsevier Limited: New York, NY, USA, 2016; ISBN 978-070-205-230-9. [Google Scholar]
- Nagy, J.A.; Chang, S.-H.; Dvorak, A.M.; Dvorak, H.F. Why are tumour blood vessels abnormal and why is it important to know? Br. J. Cancer 2009, 100, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Al Fozan, H.; Tulandi, T. Factors affecting early surgical intervention after uterine artery embolization. Obstet. Gynecol. Surv. 2002, 57, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Bilhim, T.; Pisco, J.M.; Duarte, M.; Oliveira, A.G. Polyvinyl Alcohol Particle Size for Uterine Artery Embolization: A Prospective Randomized Study of Initial Use of 350–500μm Particles versus Initial Use of 500–700 μm Particles. J. Vasc. Interv. Radiol. 2011, 22, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Es, R.J.; Franssen, O.; Dullens, H.F.; Bernsen, M.R.; Bosman, F.; Hennink, W.E.; Slootweg, P.J. The VX2 carcinoma in the rabbit auricle as an experimental model for intra-arterial embolization of head and neck squamous cell carcinoma with dextran microspheres. Lab. Anim. 1999, 33, 175–184. [Google Scholar] [PubMed]

{kind=link}
| Material Type | Acronym (If Applicable) | Standard Search Parameters |
|---|---|---|
| Poly(lactic-co-glycolic acid) | PLGA | “Material Type” ** AND “Microsphere” |
| PLGA-Polyethylene Glycol-PLGA | PLGA-PEG-PLGA | “Material Type” AND “Embolization” |
| Carboxymethylcellulose | CMC | “Material Type” AND “Occlusion” |
| Chitin | “Material Type” AND “Arterial” | |
| Hydroxyethyl acrylate | HEA | “Material Type” AND “Radiology” |
| Albumin * | “Material Type” AND “Bead” | |
| Gelatin | “Material Type” AND “Resorbable” | |
| Pluronic F127 | “Material Type” AND “Bioresorbable” | |
| Polyvinyl alcohol | PVA | “Material Type” AND “Degradable” |
| Starch | “Material Type” AND “Bioabsorbable” |
| Material Type | Initial Returned Searches | Articles Meeting Inclusion Criteria | Article Title |
|---|---|---|---|
| PLGA | 1662 | 1 | A Preclinical Study of the Safety and Efficacy of OcclusinTM 500 Artificial Embolization Device in Sheep |
| PLGA-PEG-PLGA | 985 | 2 | A Novel Resorbable Embolization Microsphere for Transient Uterine Artery Occlusion: A Comparative Study with Trisacryl-Gelatin Microspheres in the Sheep Model |
| Targeting and Recanalization after Embolization with Calibrated Resorbable Microspheres versus Hand-cut Gelatin Sponge Particles in a Porcine Kidney Model | |||
| CMC | 417 | 1 | Calibrated Bioresorbable Microspheres: A Preliminary Study on the Level of Occlusion and Arterial Distribution in a Rabbit Kidney Model |
| Chitin | 585 | 1 | Chitin-based Embolic Materials in the Renal Artery of Rabbits: Pathologic Evaluation of an Absorbable Particulate Agent |
| Hydroxyethyl acrylate | 65 | 1 | Transcatheter embolization using degradable crosslinked hydrogels |
| PVA | 2014 | 0 | |
| Albumin | 6751 | 0 | |
| Gelatin | 2347 | 0 | |
| Pluronic F127 | 41 | 0 | |
| Starch | 2083 | 0 | |
| TOTAL | 16,950 | 6 |
| Authors and Year of Publication | Study Model & Duration | Test Material Information. | Ease of Use | Time to Complete Degradation of Test Material | Recanalization | Acute Complications (Vessel Rupture/Perforation) | Local and Systemic Foreign Body Reactions | Embolization Effectiveness. | Device Migration |
|---|---|---|---|---|---|---|---|---|---|
| Owen et al. (2012) | Uterine Artery Sheep Model 32 Suffolk cross sheep (Mean weight ca. 60 kg) Study duration: 12 months. Cohorts at 1, 3, 6 and 12 months. Control material: Embosphere 300–500 μm | PLGA 150–212 μm No particle size distribution analysis is provided. | UA selectively catheterized with either 2.3F Rapid Transit or 2.3F Prowler (Cordis Corporation). Fluoroscopic time to achieve stasis was comparable for the test article (8.9 ± 2.7 min) and Embosphere (8.1 ± 3.6 min) Suspensions in “a solution of normal saline and contrast medium’ were noted as being “easily delivered to target vasculature” using a 2.3F catheter. | Test material still present at 1 and 3 months. By 6 months the authors state that no residual material was observed, but occlusion remained persistent due to the presence of fibrous connective tissue. | 3/4 animals treated with test article showed recanalization at 12 months. Recanalized vessels showed normal luminal architecture “histologically indistinguishable from the untreated contralateral vessel” No recanalization in Embosphere cohorts. | Vessel rupture not assessed. None reported. | Standard hematology and clinical chemistry parameters we performed prior to procedures, at 1, 7, 14 days, and 1, 3, 6, 12 months. No differences reported between test and control. At 1 month, fibrous connective tissue observed around test material, fully occludes treated vessels by 3 months and persists at 6 months. Vessels treated with test material were fully recanalized at 12 months and had similar architecture to untreated vessels. Microspheres of both types were embedded in a thin collagen matrix with small numbers of macrophages and occasional giant cells present. Yet inflammation was not a significant feature of the reaction to either type of microsphere. | Determined as being equivalent to Embosphere up to at least 6 months. | Not directly addressed. Histology showed test articles present in all 12 (100%) treated uterine arteries and in 1 untreated uterine artery, but not in vaginal, ovarian, or vesical vasculatures of any animal. Control articles were detected in all 16 (100%) treated uterine arteries, 6 (40%) untreated uterine arteries, as well in the vaginal vasculature of 10 (63%) animals, ovarian vasculature of 2 (13%), and Vesical vesicle vasculature of 1 (6%) animal. |
| Authors and Year of Publication | Study Model & Duration | Test Material Information. | Ease of Use | Time to Complete Degradation of Test Material | Recanalization | Acute Complications (Vessel Rupture/Perforation) | Local and Systemic Foreign Body Reactions | Embolization Effectiveness. | Device Migration |
|---|---|---|---|---|---|---|---|---|---|
| Maeda et al. (2013) | Porcine Kidney Model. Study duration: 7 days. Control material: gelatin sponge particle (GSP) approx. 1 mm3 9 Minipigs (Mean weight 34.9 kg ± 2.1 kg) Groups comprised two pigs (i.e., four kidneys per group) | PEG-PLGA-PEG 300–500 μm 500–700 μm 700–900 μm Size distributions determined by sieving only. No particle size distribution analysis is provided. 1:2 ratio of saline/contrast for test article with pure contrast for the control article | A 4-F cobra catheter was utilized for the embolization procedures. The mean volume of injected material per kidney was 0.48 mL ± 0.17, 0.24 mL ± 0.11, 0.24 mL ± 0.12 for REM of 300–500 μm, 500–700 μm, and 700–900 μm. Mean volume of control article injected was 1.2 mL ± 0.2 Authors note, “none of the products clogged in the catheter.” | Proposed as 24 h based on tests in PBS. At day 7 the test material was not visible, no fragments of materials were observed in histological slides/analysis. GSP was still present at day 7, though partly degraded. Its presence was associated with foreign body inflammation. | Assessed at 10 min and 7 days using angiography. Large variations due to methodology acknowledged. Assessed at 10 min and 7 days using histological analysis. At day 0 test materials were washed out during processing limiting analysis. Test article showed fully patent vessel lumens after 7 days Recanalization varied based on size of test material: 700–900 μm demonstrated complete recanalization 300–500 μm and 500–700 μm demonstrated partial recanalization. | Numerous patchy arterial lesions, including myointimal proliferation, medial concentric thickening, adventitial fibrosis, and fibrinoid necrosis of the arterial wall, were focally observed. No excessive pain or abnormal behavior reported | Local histological analysis provided. Hematoxylin-eosin-saffron stain used. GSP (control) had eosinophilic or slightly basophilic appearance at day 7 and partly degraded. Presence associated with foreign body inflammation (macrophages, lymphocytes and fibrocytes). Test materials were washed out during histological processing limiting analysis for day 0. At day 7, test material was not visible, no fragments of materials were observed in histological slides/analysis. Fully patent lumen visible on histology. | Recanalization demonstrated on angiography No gross histology to examine presence of long term necrosis | Not addressed. |
| Verret et al. (2014) | Uterine Artery Sheep Model 6 adult Préalpes Sheep. (Mean weight 54 kg) (Mean age 48 ± 22 months) Study duration: 7 days. Control material: Embosphere 500–700 μm | PEG-PLGA-PEG 500–700 μm Size distributions determined by sieving only. No particle size distribution analysis is provided. 2:1 ration of saline/contrast for test material and 4:5 ratio for control article | Selective embolization of both internal iliac arteries achieved using a 5F “cobra-type” catheter. Superselective embolization of both UAs performed with a 2.7F microcatheter. Mean volume of test material injected per uterine artery was 1.0 mL ± 0.5. Mean volume of control was 1.6 mL ± 0.9 No difference in injectability noted between control and test materials. | Proposed as 24hr based on tests in PBS. At day 7 the test material was not visible, no fragments of materials were observed in histological slides/analysis. | Presence or absence of recanalization assessed based on (i) the presence or absence of vascular lumen with (ii) red blood cells or plasma in the occluded vessel. For test article “complete recanalization rapidly obtained” and fully patent on angiography at 7 days. | Vessel rupture not assessed. None reported. | Local histological analysis provided. Gross examination showed ischemic damage to endometrium and myometrium for test and control uteri. Hematoxylin-eosin-saffron stain used. No test materials or inflammatory response observed at 7 days for test article. Control material showed evidence of recanalization, and was surrounded by macrophages, neutrophils and foreign body giant cells. | Gross examination showed ischemic damage to endometrium and myometrium for test and control uteri. The authors suggest that for the test article, full UA recanalization and absence of parenchymal defects were associated with low endometrial alterations. | Not addressed. |
| Authors and Year of Publication | Study Model & Duration | Test Material Information. | Ease of Use | Time to Complete Degradation of Test Material | Recanalization | Acute Complications (Vessel Rupture/Perforation) | Local and Systemic Foreign Body Reactions | Embolization Effectiveness. | Device Migration |
|---|---|---|---|---|---|---|---|---|---|
| Weng et al. (2013) | Renal Artery Rabbit Model 11 New Zealand white rabbits (Weight range 4–5 kg) 3 rabbits (group 1) received partial occlusion with BRMS-I (3, 15, and 25 mg of microspheres) To test the level of occlusion, 4 (group 2) received total occlusion with BRMS-I (10 mg/mL), and 4 more (group 3) rabbits received complete occlusion with BRMS-II Study duration: 15 min Tris-acryl gelatin microspheres (TGMS) (100–300 μm) were used as a control | 2 test articles: BRMS-I and BRMS-II 2% (w/v) oxidized carboxymethylcellulose and 2% (w/v) carboxymethyl chitosan 10% oxidized carboxymethylcellulose was used in BRMS-I and 25% oxidized carboxymethylcellulose was used in BRMS-II 100–300 μm Average diameter of the microspheres was 250 μm ± 50 for BRMS-I, and 255 μm ± 45 for BRMS-II Concentration of microsphere suspension used was 1 mg/mL and 5 mg/mL for group 1, and 10 mg/mL for groups 2 and 3 all in a 5:5 saline:contrast solution | RA selectively catheterized a 4-F Cobra catheter inside which a 2.8-F microcatheter was placed Injection was “easily performed without any clogging or clumping” BRMS were deemed to be less “sticky” than TGMS BRMS-I required 8.7 mL ± 3.5 to achieve stasis and BRMS-II required 6.3 mL ± 0.8 Fluoroscopic time to achieve the endpoint was 4.5 min ± 1.6 for BRMS-I and 3.8 min ± 0.74 | Not Addressed | Not addressed | Not addressed | Not addressed | Determined to achieve the desired goal of embolization similar to commercially available TGMS Mean diameter of occluded vessels found to be 197 μm ± 23 for BRMS-I, 219 μm ±36 for BRMS-II and 158 μm ±21 for TGMS | Not addressed |
| Authors and Year of Publication | Study Model & Duration | Test Material Information. | Ease of Use | Time to Complete Degradation of Test Material | Recanalization | Acute Complications (Vessel Rupture/Perforation) | Local and Systemic Foreign Body Reactions | Embolization Effectiveness. | Device Migration |
|---|---|---|---|---|---|---|---|---|---|
| Kwak et al. (2005) | Renal Artery Rabbit Model 36 New Zealand white rabbits (weight range 2.0–3.5 kg) Study duration: 32 weeks. Cohorts at 1 and 3 days, and 1, 2, 4, 8, 16, 24, and 32 weeks Control material: PVA 150–250 μm | Chitin particles, 99% deacetylated chitosan particles, and 75% deacetylated chitosan microspheres 150–250 μm The length of chitin particles, chitosan particles, and chitosan microspheres was 335 μm ± 56.8, 466 μm ± 100.2, and 271 μm ± 37.2, respectively | RA selectively catheterized with 4-F angiography cobra catheter. No fluoroscopic time to achieve stasis given All four materials were noted as being “easily injected through the catheter without causing any blockage” | All embolic materials maintained their shape until week 8 Chitin particles showed fragmentation and absorption at week 24, absorbed completely at week 32 Chitosan particles showed fragmentation and absorption at week 16, absorbed completely by week 24 Chitosan microspheres showed degradation and absorptionat week 24, absorbed completely by week 32 | Severe proliferations of the blood vessels by the retroperitoneal fat around the embolized kidney were observed from day 1 to week 1 for PVA, chitin and chitosan microspheres and from day 3 to week 2 for chitosan particles. Formation of capillaries were observed most frequently with PVA particles, followed by chitosan particles and chitosan microspheres | The degree of vascular injuries was moderately reactive with PVA particles and chitosan microspheres and substantially reactive with chitin particles No hemorrhage or extravasation for any of the embolic materials. | Giant cell reaction appeared prominently 1–2 weeks after embolization, and lasted until week 32. The degree of reaction was lowest with chitosan microspheres. As a whole, there was no substantial difference in gross observations among the four groups. | Chitosan microspheres were determined to be potential embolic agents as they block the blood vessels more compactly and with a lower rate of capillary formation than PVA particles. | Not addressed. |
| Authors and Year of Publication | Study Model & Duration | Test Material Information. | Ease of Use | Time to Complete Degradation of Test Material | Recanalization | Acute Complications (Vessel Rupture/Perforation) | Local and Systemic Foreign Body Reactions | Embolization Effectiveness. | Device Migration |
|---|---|---|---|---|---|---|---|---|---|
| Schwarz et al. (2003) | Renal Artery Canine Model 5 Beagles (Weight range 10–15 kg) 3 Kidneys were embolized with HEA Median auricular artery occlusion model 5 New Zealand rabbits (Weight range 2.5–3.5 kg) 4 central auricular arteries were embolized with HEA microspheres Study duration: 3 weeks. Monitored immediate and weekly through catheter angiography Control material: EmboGold microspheres 300–500 μm | Hydroxyethyl acrylate 300–500 μm No particle size distribution analysis is provided. | RA selectively catheterized with either 4-F or 5-F catheters. Catheterization of central artery of rabbit ears was performed with radiopaque catheters No comment made on ease of use | At 3 weeks, microspheres (sometimes intact but encapsulated, most often in various stages of degradation and phagocytosis) could be detected Occlusion lasted for the critical period at risk for recanalization, typically 10–14 days | Renal arterial occlusions that persisted at 1 week were recanalized at 3 weeks Experiments performed in the rabbit central auricular arterial model showed that HEA microspheres led to occlusions that persisted at 1 week but that recanalized at 2 weeks No recanalization in EmboGold cohorts. | Vessel rupture not assessed. None reported. | Only a residual inflammatory reaction and some neointimal thickening could be observed as a witness to the previous presence of these degradable microspheres | Determined as being potentially effective up to 2 weeks | Not addressed. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doucet, J.; Kiri, L.; O’Connell, K.; Kehoe, S.; Lewandowski, R.J.; Liu, D.M.; Abraham, R.J.; Boyd, D. Advances in Degradable Embolic Microspheres: A State of the Art Review. J. Funct. Biomater. 2018, 9, 14. https://doi.org/10.3390/jfb9010014
Doucet J, Kiri L, O’Connell K, Kehoe S, Lewandowski RJ, Liu DM, Abraham RJ, Boyd D. Advances in Degradable Embolic Microspheres: A State of the Art Review. Journal of Functional Biomaterials. 2018; 9(1):14. https://doi.org/10.3390/jfb9010014
Chicago/Turabian StyleDoucet, Jensen, Lauren Kiri, Kathleen O’Connell, Sharon Kehoe, Robert J. Lewandowski, David M. Liu, Robert J. Abraham, and Daniel Boyd. 2018. "Advances in Degradable Embolic Microspheres: A State of the Art Review" Journal of Functional Biomaterials 9, no. 1: 14. https://doi.org/10.3390/jfb9010014