Virtual Reality Treatment for Public Speaking Anxiety in Students. Advancements and Results in Personalized Medicine

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
- (i)
- Analysis of VR exposure attrition rate and in vivo exposure therapy. The review collected 46 studies. The meta-analysis obtained concise data that both therapies show similar attrition rates [32].
- (ii)
- Applicability of VR to mental health disorders. Twenty-nine studies were identified that applied VR for anxiety disorders, depression, schizophrenia, psychosis, eating disorders, and obsessive-compulsive disorder [33].
- (iii)
- Effectiveness of VRET for social anxiety. The meta-analysis results of the six studies analyzed showed a significant overall effect size. Thus, VRET was effective in reducing social anxiety [34].
- (iv)
- Analysis of VR interventions for anxiety, depression, and treatment wasting outcomes. Meta-analysis results showed that VR interventions overcame control conditions for anxiety and depression, but did not improve desertion from treatment [35].
- (v)
- Applicability of VR to health problems. Fifty studies were analyzed where different VR uses were detected to treat problems related to fear of flying, PSA, arachnophobia, agoraphobia, body image disturbance, and obesity [36].
- (vi)
- Effectiveness of VRET for the treatment of anxiety disorders. The analysis found that VRET is effective for the treatment of anxiety, phobias, panic disorder, and post-traumatic stress disorder [37].
- (vii)
- Effectiveness of VRET for anxiety-related disorders. Forty-nine studies were included where the majority reported positive findings in favor of VRET [38].
- (viii)
- Comparison of the efficacy of VRET with classic treatments for anxiety. The 23 studies identified concluded in the meta-analysis that VRET is equally as effective as classical treatments, with no differences in dropout rate or stability of results over time [39].
- (ix)
- Reduction of anxiety of different types (social phobia, arachnophobia, agoraphobia, acrophobia, aviophobia) through the VRET. Twenty-one studies were reviewed that found that anxiety symptoms were diminished with VR treatment [40].
- (x)
- Measurement of the size of the effect of VR for the treatment of anxiety disorders. The meta-analysis collected a large average effect size for VRET compared with in vivo exposure and control conditions [41].
- RQ1. How many studies were published over the years?
- RQ2. Who are the most active authors in the area?
- RQ3. In which sources appear this kind of study?
- RQ4. What is the educational stage and the country of the students?
- RQ5. How long was the treatment and what sequence was used?
2. Methods
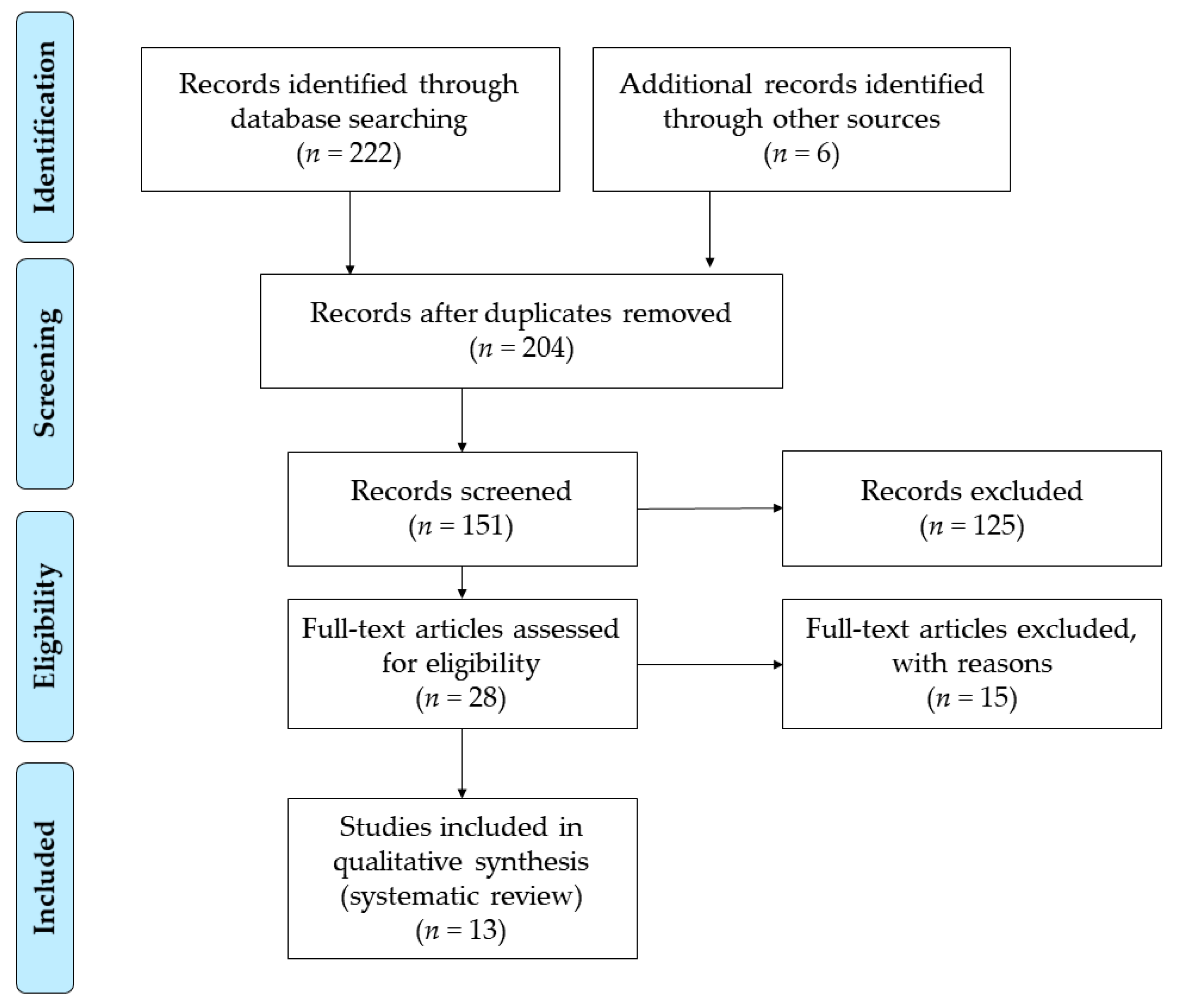
2.1. Search Strategy
2.2. Data Collection and Analysis
3. Results
3.1. RQ1. How Many Studies were Published over the Years?
3.2. RQ2. Who are the Most Active Authors in the Area?
3.3. RQ3. In Which Sources Appear this Kind of Studies?
3.4. RQ4. What is the Educational Stage and the Country of the Students?
3.5. RQ5. How Long was the Treatment and what Sequence was Used?
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Safir, M.P.; Wallach, H.S.; Bar-Zvi, M. Virtual Reality Cognitive-Behavior Therapy for Public Speaking Anxiety: One-Year Follow-Up. Behav. Modif. 2012, 36, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Ruscio, A.M.; Brown, T.A.; Chiu, W.T.; Sareen, J.; Stein, M.B.; Kessler, R.C. Social fears and social phobia in the USA: Results from the National Comorbidity Survey Replication. Psychol. Med. 2008, 38, 15–28. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association (APA). DSM-V: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Anderson, P.L.; Rothbaum, B.O.; Hodges, L.F. Virtual Reality Exposure in the Treatment of Social Anxiety. Cogn. Behav. Pract. 2003, 10, 240–247. [Google Scholar] [CrossRef]
- Liao, J.A.; Jincho, N.; Kikuchi, H. Interactive Virtual Reality Speech Simulation System Using Autonomous Audience with Natural non-Verbal Behavior. Int. J. Mach. Learn. Comput. 2018, 8, 404–407. [Google Scholar]
- Myers, C.E.; Kostek, J.A.; Ekeh, B.; Sánchez, R.; Ebanks-Williams, Y.; Krusznis, A.; Weinflash, N.; Servatius, R.J. Watch what I do, not what I say I do: Computer-based avatars to assess behavioural inhibition, a vulnerability factor for anxiety disorders. Comput. Hum. Behav. 2016, 55, 804–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, C.; Ling, Y.; Heynderickx, I.; Brinkman, W.P. Virtual Bystanders in a Language Lesson: Examining the Effect of Social Evaluation, Vicarious Experience, Cognitive Consistency and Praising on Students’ Beliefs, Self-Efficacy and Anxiety in a Virtual Reality Environment. PLoS ONE 2015, 10, e0125279. [Google Scholar] [CrossRef]
- Metsis, V.; Lawrence, G.; Trahan, M.; Smith, K.S.; Tamir, D.; Selber, K. 360 Video: A prototyping process for developing virtual reality interventions. J. Technol. Hum. Serv. 2019, 37, 1–19. [Google Scholar] [CrossRef]
- Cohen, S. Social Relationships and Health. Am. Psychol. 2004, 59, 676–684. [Google Scholar] [CrossRef]
- Hardie, E.; Tee, M.Y. Excessive Internet Use: The Role of Personality, Loneliness and Social Support Networks in Internet Addiction. Aust. J. Emerg. Techno. Soc. 2007, 5, 34–47. [Google Scholar]
- Ruiz-Palmero, J.; Sánchez-Rodríguez, J.; Gómez-García, M.; Sánchez, E. Future Teachers’ Smartphone Uses and Dependence. Educ. Sci. 2019, 9, 194. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.L.; Edwards, S.M.; Goodnight, J.R. Virtual Reality and Exposure Group Therapy for Social Anxiety Disorder: Results from a 4–6 Year Follow-Up. Cognit. Ther. Res. 2017, 41, 230–236. [Google Scholar] [CrossRef]
- Price, M.; Anderson, P.L. Outcome Expectancy as a Predictor of Treatment Response in Cognitive Behavioral Therapy for Public Speaking Fears Within Social Anxiety Disorder. Psychotherapy 2012, 49, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Scozzari, S.; Gamberini, L. Virtual Reality as a Tool for Cognitive Behavioral Therapy: A Review. In Advanced Computational Intelligence Paradigms in Healthcare 6. Virtual Reality in Psychotherapy, Rehabilitation, and Assessment; Brahnam, S., Jain, L.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Šalkevicius, J.; Miškinyte, A.; Navickas, L. Cloud Based Virtual Reality Exposure Therapy Service for Public Speaking Anxiety. Information 2019, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.L.; Zimand, E.; Hodges, L.F.; Rothbaum, B.O. Cognitive behavioral therapy for public-speaking anxiety using virtual reality for exposure. Depress. Anxiety 2005, 22, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Klinger, E.; Bouchard, S.; Légeron, P.; Roy, S.; Lauer, F.; Chemin, I.; Nugues, P. Virtual Reality Therapy Versus Cognitive Behavior Therapy for Social Phobia: A Preliminary Controlled Study. Cyberpsychol. Behav. 2005, 8, 76–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Repetto, C.; Riva, G. From virtual reality to interreality in the treatment of anxiety disorders. Neuropsychiatry 2011, 1, 31–43. [Google Scholar] [CrossRef] [Green Version]
- Brundage, S.B.; Hancock, A.B. Real Enough: Using Virtual Public Speaking Environments to Evoke Feelings and Behaviors Targeted in Stuttering Assessment and Treatment. Am. J. Speech Lang. Pathol. 2015, 24, 139–149. [Google Scholar] [CrossRef]
- Kampmann, I.L.; Emmerlkamp, P.M.G.; Hartanto, D.; Brinkman, W.P.; Zijlstra, B.J.H.; Morina, N. Exposure to virtual social interactions in the treatment of social anxiety disorder: A randomized controlled trial. Behav. Res. Ther. 2016, 77, 147–156. [Google Scholar] [CrossRef]
- Yuen, E.K.; Goetter, E.M.; Stasio, M.J.; Ash, P.; Mansour, B.; McNally, E.; Sánchez, M.; Hobar, E.; Forte, S.; Zulaica, K.; et al. A pilot of acceptance and commitment therapy for public speaking anxiety delivered with group videoconferencing and virtual reality exposure. J. Contextual Behav. Sci. 2019, 12, 47–54. [Google Scholar] [CrossRef]
- Schmid, M.; Kleinlogel, E.P.; Tur, B.; Bachmann, M. The future of interpersonal skills development: Immersive virtual reality training with virtual humans. Hum. Resour. Dev. Q. 2018, 29, 125–141. [Google Scholar] [CrossRef]
- Takac, M.; Collett, J.; Blom, K.J.; Conduit, R.; Rehm, I.; De Foe, A. Public speaking anxiety decreases within repeated virtual reality training sessions. PLoS ONE 2019, 14, e0216288. [Google Scholar] [CrossRef] [Green Version]
- North, M.M.; North, S.M.; Coble, J.R. Virtual Reality Therapy: An Effective Treatment for Psychological Disorders. In Virtual Reality in Neuro-Psycho-Physiology.; Riva, G., Ed.; Ios Press: Amsterdam, The Netherlands, 1997. [Google Scholar]
- Anderson, P.L.; Price, M.; Edwards, S.M.; Obasaju, M.A.; Schmertz, S.K.; Zimand, E.; Calamaras, M.R. Virtual Reality Exposure Therapy for Social Anxiety Disorder: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2013, 81, 751–760. [Google Scholar] [CrossRef]
- Bouchard, S.; Dumoulin, S.; Robilard, G.; Guitard, T.; Klinger, E.; Forget, H.; Loranger, C.; Roucaut, F.X. Virtual reality compared with in vivo exposure in the treatment of social anxiety disorder: A three-arm randomised controlled trial. Br. J. Psychiatry 2017, 210, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Ryan, V.; Griffin, R. An Investigation into Anxiety In Virtual Reality Following A Self-Compassion Induction. Annu. Rev. CyberTher. Telemed. 2016, 14, 109–114. [Google Scholar]
- Wallach, H.S.; Safir, M.P.; Bar-Zvi, M. Virtual Reality Exposure versus Cognitive Restructuring for Treatment of Public Speaking Anxiety: A Pilot Study. Isr. J. Psychiatry Relat. Sci. 2011, 48, 91–97. [Google Scholar] [PubMed]
- Cheng, K.H.; Tsai, C.C. A case study of immersive virtual field trips in an elementary classroom: Students’ learning experience and teacher-student interaction behaviors. Comput. Educ. 2019, 140, 103600. [Google Scholar] [CrossRef]
- Kardong-Edgren, S.; Breitkreuz, K.; Werb, M.; Foreman, S.; Ellertson, A. Evaluating the usability of a second-generation virtual reality game for refreshing sterile urinary catheterization skills. Nurse Educ. 2019, 44, 137–141. [Google Scholar] [CrossRef]
- Otkhmezuri, B.; Boffo, M.; Siriaraya, P.; Matsangidou, M.; Wiers, R.W.; Mackintosh, B.; Ang, C.S.; Salemink, E. Believing Is Seeing: A Proof-of-Concept Semiexperimental Study on Using Mobile Virtual Reality to Boost the Effects of Interpretation Bias Modification for Anxiety. JMIR Ment. Health 2019, 6, e11517. [Google Scholar] [CrossRef] [PubMed]
- Benbow, A.A.; Anderson, P.L. A meta-analytic examination of attrition in virtual reality exposure therapy for anxiety disorders. J. Anxiety Disord. 2019, 61, 18–26. [Google Scholar] [CrossRef]
- Brito, H.C.; Vicente, B.P. Virtual reality and its applications in mental disorders: A review. Rev. Chil. Neuropsiquiatr. 2018, 56, 127–135. [Google Scholar]
- Chesham, R.K.; Malouff, J.M.; Schutte, N.S. Meta-Analysis of the Efficacy of Virtual Reality Exposure Therapy for Social Anxiety. Behav. Chang. 2018, 35, 152–166. [Google Scholar] [CrossRef] [Green Version]
- Fodor, L.A.; Cotet, C.D.; Cuijpers, P.; Szamoskozi, S.; David, D.; Cristea, I.A. The effectiveness of virtual reality based interventions for symptoms of anxiety and depression: A meta-analysis. Sci. Rep. 2018, 8, 10323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregg, L.; Tarrier, N. Virtual reality in mental health. A review of the literature. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 343–354. [Google Scholar] [CrossRef]
- Meyerbroker, K.; Emmelkamp, P.M.G. Virtual reality exposure therapy in anxiety disorders: A systematic review of process-and-outcome studies. Depress. Anxiety 2010, 27, 933–944. [Google Scholar] [CrossRef]
- Oing, T.; Prescott, J. Implementations of Virtual Reality for Anxiety-Related Disorders: Systematic Review. J. Med. Internet Res. 2018, 20, e10965. [Google Scholar] [CrossRef]
- Opris, D.; Pintea, S.; García-Palacios, A.; Botella, C.; Szamoskozi, S.; David, D. Virtual reality exposure therapy in anxiety disorders: A quantitative meta-analysis. Depress. Anxiety 2012, 29, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D.; Rizzo, A.A. Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: A meta-analysis. J. Behav. Ther. Exp. Psychiatry 2008, 39, 250–261. [Google Scholar] [CrossRef]
- Powers, M.B.; Emmelkamp, P.M.G. Virtual reality exposure therapy for anxiety disorders: A meta-analysis. J. Anxiety Disord. 2008, 22, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Hedges, L.V.; Olkin, I. Statistical Models for Meta-Analysis; Academic Press: New York, NY, USA, 1985. [Google Scholar]
- Marín, F.; Sánchez, J.; López, J.A. Meta-analysis in the Health Sciences: An indispensable methodology for the efficient accumulation of knowledge. Fisioterapia. 2009, 31, 107–114. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzla, J.; Altman, D.G. PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Benito, J.; García-Peñalvo, F.J.; Therón, R. Analyzing the software architectures supporting HCI/HMI processes through a systematic review of the literature. Telemat. Inform. 2019, 38, 118–132. [Google Scholar] [CrossRef]
- Aznar, I.; Cáceres, M.P.; Romero, J.M. Effect of the mobile learning methodology in university education: Meta-analysis of the research published in WOS and Scopus. RISTI 2018, 30, 1–16. [Google Scholar]
- Denizci, M.; Yilmaz, M.; Gulec, U.; Yilmaz, A.E.; Isler, V.; O’Connor, R.V.; Gozcu, M.A.; Claske, P. Interactive three-dimensional virtual environment to reduce the public speaking anxiety levels of novice software engineers. IET Softw. 2019, 13, 152–158. [Google Scholar]
- Dubiago, M.; Poeschl, S.; Doering, N. Influence of Simulation Fidelity on Perceived Simulation Realism – An Exploratory Study on a Virtual Public Speaking Training Application. Annu. Rev. CyberTher. Telemed. 2017, 15, 154–159. [Google Scholar]
- Harris, S.R.; Kemmerling, R.L.; North, M.M. Brief Virtual Reality Therapy for Public Speaking Anxiety. Cyberpsychol. Behav. Soc. Netw. 2002, 5, 543–550. [Google Scholar] [CrossRef]
- Heuett, B.L.; Heuett, K.B. Virtual Reality Therapy: A Means of Reducing Public Speaking Anxiety. Int. J. Humanit. Soc. Sci. 2011, 1, 1–6. [Google Scholar]
- Kahlon, S.; Lindner, P.; Nordgreen, T. Virtual reality exposure therapy for adolescents with fear of public speaking: A non-randomized feasibility and pilot study. Child. Adolesc. Psychiatry Ment. Health 2019, 13, 47. [Google Scholar] [CrossRef]
- Lindner, P.; Miloff, A.; Fagernäs, S.; Andersen, J.; Sigeman, M.; Andersson, G.; Furmark, T.; Carlbring, P. Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: A randomized controlled trial. J. Anxiety Disord. 2019, 61, 45–54. [Google Scholar] [CrossRef]
- Morina, N.; Brinkman, W.P.; Hartanto, D.; Kampmann, I.L.; Emmelkamp, P.M.G. Social interactions in virtual reality exposure therapy: A proof-of-concept pilot study. Technol. Health Care 2015, 23, 581–589. [Google Scholar] [CrossRef] [Green Version]
- North, M.M.; Hill, J.; Aikhuele, A.S.; North, S.M. Virtual Reality Training in Aid of Communication Apprehension in Classroom Environments. Int. J. Emerg. Techno. Learn. 2008, 3, 34–37. [Google Scholar]
- Parrish, D.E.; Oxhandler, H.K.; Duron, J.F.; Swank, P.; Bordnick, P. Feasibility of Virtual Reality Environments for Adolescent Social Anxiety Disorder. Res. Soc. Work Pract. 2016, 26, 825–835. [Google Scholar] [CrossRef]
- Poeschl, S. Virtual reality Training for Public speaking—A QUEST-VR Framework Validation. Front. ICT 2017, 4, 13. [Google Scholar] [CrossRef]
- Poeschl, S.; Doering, N. Effects of Simulation Fidelty on User Experience in Virtual Fear of Public Speaking Training—An Experimental Study. Annu. Rev. CyberTher. Telemed. 2014, 199, 66–70. [Google Scholar]
- Stupar-Rutenfrans, S.; Ketelaars, L.E.H.; Van Gisbergen, M.S. Beat the Fear of Public Speaking: Mobile 360° Video Virtual Reality Exposure Training in Home Environment Reduces Public Speaking Anxiety. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Wilsdon, L.; Fullwood, C. The Effect of Immersion and Presence in a Virtual Reality Public Speaking Task. Annu. Rev. CyberTher. Telemed. 2017, 17, 211–213. [Google Scholar]



{kind=link}
{kind=link}
| Inclusion Criteria (IC) | Exclusion Criteria (EX) |
|---|---|
| IC1: Journal articles. | EX1: Proceedings of congresses, book chapters, books, or other types of non-peer-reviewed publications. |
| IC2: Empirical research. | EX2: Theoretical studies or revisions. |
| IC3: The papers are written in English language. | EX3: The papers are not described in English. |
| IC4: Using Virtual Reality as a treatment for public speaking anxiety. | EX4: Virtual Reality is not used as a treatment for public speaking anxiety. |
| IC5: Population are students. | EX5: The study population are not students. |
| Database | Search Descriptors | Papers |
|---|---|---|
| WoS | TS = (“Virtual reality” AND anxiety AND “Public speaking”). Time period = Every year. Index = SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC. | 139 |
| SCOPUS | TITLE-ABS-KEY ("virtual reality" OR VR) AND TITLE-ABS-KEY (anxiety) AND TITLE-ABS-KEY ("public speaking"). Time period = Every year. | 83 |
| Author | Total |
|---|---|
| Poeschl, S. | 3 |
| Doering, N., Lindner, P., North, M.M. | 2 |
| Aikhuele, A.S., Andersen, J., Andersson, G., Bordnick, P., Brinkman, W.P., Carlbring, P., Claske, P., Denizci, M., Dubiago, M., Duron, J.F., Emmelkamp, P.M.G., Fagernäs, S., Fullwood, C., Furmark, T., Gozcu, M.A., Gulec, U., Harris, S.R., Hartanto, D., Heuett, B.L., Heuett, K.B., Hill, J., Isler, V., Kahlon, S., Kampmann, I.L., Kemmerling, R.L., Ketelaars, L.E.H., Miloff, A., Morina, N., Nordgreen, T., North, S.M., O’Connor, R.V., Oxhandler, H.K., Parrish, D.E., Sigeman, M., Stupar-Rutenfrans, S., Swank, P., Van Gisbergen, M.S., Wilsdon, L., Yilmaz, A.E., Yilmaz, M. | 1 |
| Reference | Journal | h-Index |
|---|---|---|
| [49,58,60] | Annual Review of Cybertherapy and Telemedicine | 8 |
| [50,59] | Cyberpsychology, Behavior, and Social Networking | 50 |
| [57] | Frontiers in ICT | 15 |
| [48] | IET Software | 13 |
| [55] | International Journal of Emerging Technologies in Learning | 19 |
| [53] | International Journal of Humanities and Social Science | 4 |
| [56] | Research on Social Work Practice | 27 |
| [54] | Technology and Health Care | 18 |
| [51] | Child and Adolescent Psychiatry and Mental Health | 26 |
| [52] | Journal of Anxiety Disorders | 47 |
| Reference | Educational Stage | n | Age (M) | Country | |
|---|---|---|---|---|---|
| High School | University | ||||
| Denizci et al. (2019) [48] | X | 14 | 21.36 | Turkey | |
| Dubiago et al. (2017) [49] | X | 40 | 25.60 | Germany | |
| Harris et al. (2002) [50] | X | 14 | - | USA | |
| Heuett and Heuett (2011) [51] | X | 80 | 20 | USA | |
| Kahlon et al. (2019) [52] | X | 27 | 14.22 | Norway | |
| Lindner et al. (2019) [53] | X | 50 | 31.36 | Sweden | |
| Morina et al. (2015) [54] | X | 34 | 22.3 | Netherlands | |
| North et al. (2008) [55] | X | 30 | - | Georgia | |
| Parrish et al. (2016) [56] | X | 41 | 16 | USA | |
| Poeschl (2017) [57] | X | 36 | 26.42 | Germany | |
| Poeschl and Doering (2014) [58] | X | 40 | 24 | Germany | |
| Stupar-Rutenfrans, et al. (2017) [59] | X | 35 | - | Netherlands | |
| Wilsdon and Fullwood (2017) [60] | X | 40 | 25.5 | UK | |
| No. of Reference | Social Anxiety Disorder Diagnosis | Time Pre-Post Used in Analysis | No. of Treatment Sessions (Minutes) | Assignment | Content Exposed | Favour Effect |
|---|---|---|---|---|---|---|
| [48] | Yes | 4 weeks | 4 (8–10’) | Random | Auditorium | VRET |
| [49] | No | - | 1 (5–6’) | Participant matching | Virtual classroom | VRET |
| [50] | No | 4 weeks | 4 (15’) | Random | Auditorium | VRET |
| [51] | No | 1 week | 1 (10–20’) | Quasi-random | Auditorium | VRET |
| [52] | Yes | 1 day | 1 (90’) | Participant matching | Virtual classroom | VRET |
| [53] | No | 4 weeks | 4 (20–30’) | Random | Auditorium, Meeting room and wedding reception | VRET |
| [54] | No | 12 weeks | 12 (30’) | Quasi-random | Everyday situations | VRET |
| [55] | No | 5 weeks | 4 (40–45’) | Participant matching | Auditorium | VRET |
| [56] | Yes | 1 day | 4 (5’) | Quasi-random | Party and presentation environment | VRET |
| [57] | No | 1 day | 2 (5’) | Participant matching | Virtual classroom | No effect |
| [58] | No | 1 day | 2 (5’) | Participant matching | Virtual classroom | No effect |
| [59] | No | 4 weeks | 3 (5’) | Participant matching | Virtual classroom | VRET |
| [60] | No | 1 day | 1 (5’) | Participant matching | Virtual classroom | No effect |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hinojo-Lucena, F.-J.; Aznar-Díaz, I.; Cáceres-Reche, M.-P.; Trujillo-Torres, J.-M.; Romero-Rodríguez, J.-M. Virtual Reality Treatment for Public Speaking Anxiety in Students. Advancements and Results in Personalized Medicine. J. Pers. Med. 2020, 10, 14. https://doi.org/10.3390/jpm10010014
Hinojo-Lucena F-J, Aznar-Díaz I, Cáceres-Reche M-P, Trujillo-Torres J-M, Romero-Rodríguez J-M. Virtual Reality Treatment for Public Speaking Anxiety in Students. Advancements and Results in Personalized Medicine. Journal of Personalized Medicine. 2020; 10(1):14. https://doi.org/10.3390/jpm10010014
Chicago/Turabian StyleHinojo-Lucena, Francisco-Javier, Inmaculada Aznar-Díaz, María-Pilar Cáceres-Reche, Juan-Manuel Trujillo-Torres, and José-María Romero-Rodríguez. 2020. "Virtual Reality Treatment for Public Speaking Anxiety in Students. Advancements and Results in Personalized Medicine" Journal of Personalized Medicine 10, no. 1: 14. https://doi.org/10.3390/jpm10010014