1. Introduction
Remote patient monitoring is becoming more common across the healthcare industry around the world and particularly in the United States with various medical conditions tracked when patients are away from the hospital. Wireless Medical Sensor Networks (MSNs) are cyber-physical systems (CPS) that have emerged as key building blocks to provide real-time and ubiquitous remote patient monitoring. This technology could potentially reduce the number of hospital admissions if adopted across the healthcare industry. It could also boost health outcomes, as certain medical issues could be addressed more quickly before a condition escalates. Hence, healthcare remote monitoring solutions could potentially lower medical costs across the country. Since communications between the medical staff and the devices that are monitoring the patient take place over the Internet, they are vulnerable to a variety of cyber attacks [
1].
The excessive network resources, real-time response and smart monitoring with early notifications about the patients’ status are some of the requirements to be supported. The most effective and cost-efficient solution to achieve the aforementioned requirements is to deploy MSNs, also referred to as Wireless Body Area Networks (WBANs) [
2,
3]. Typically an MSN consists of sensors or actuators that are attached in, on or in the vicinity of a human body and that operate under the control of a master node that is often referred to as a smart device. The sensors report data to the medical staff on a periodic basis on a variety of body health indicators, such as blood pressure, temperature, heart rate,
etc. The actuators execute therapeutic commands issued by the medical staff or an intelligent controller.
To overcome MSNs’ limitations (in computational power, data/energy storage and communication range/bandwidth) as standalone systems, MSNs have been integrated with cloud computing [
4]. Moreover, storing and processing the reported data at local medical units limit its accessibility and complicates the system design [
5]. Hence, integrating cloud computing with health-related systems comes to promote the gained performance by utilizing the abundant resources of data processing and storage offered by the cloud [
6,
7,
8]. In fact, cloud computing-based mobile health monitoring is claimed to be 10-times more energy-efficient and almost 20-times faster than a standalone mobile health monitoring application [
7].
Several challenges are facing this integration, including congestion, interference and coexistence issues, fast response, smart processing of the reported health-related data, supporting the maximum possible number of users, in addition to flexibility in operation and, most importantly, security [
4,
9,
10,
11]. In fact, data security is the largest obstacle that may impede the extensive usage of cloud-based MSNs. The researchers in [
8] emphasized the importance of defining system-wide security mechanisms in human-centered systems to guarantee people’s privacy. Moreover, the researchers in [
10,
12] highlighted that security and privacy are amongst the most challenging issues for mobile cloud computing. It was also reported that the patient’s health could be seriously threatened by a malicious adversary [
13], and using traditional security techniques may not be suitable, as it is recommended to offload the heavy security processing to the cloud or adopt lightweight cryptography [
14,
15].
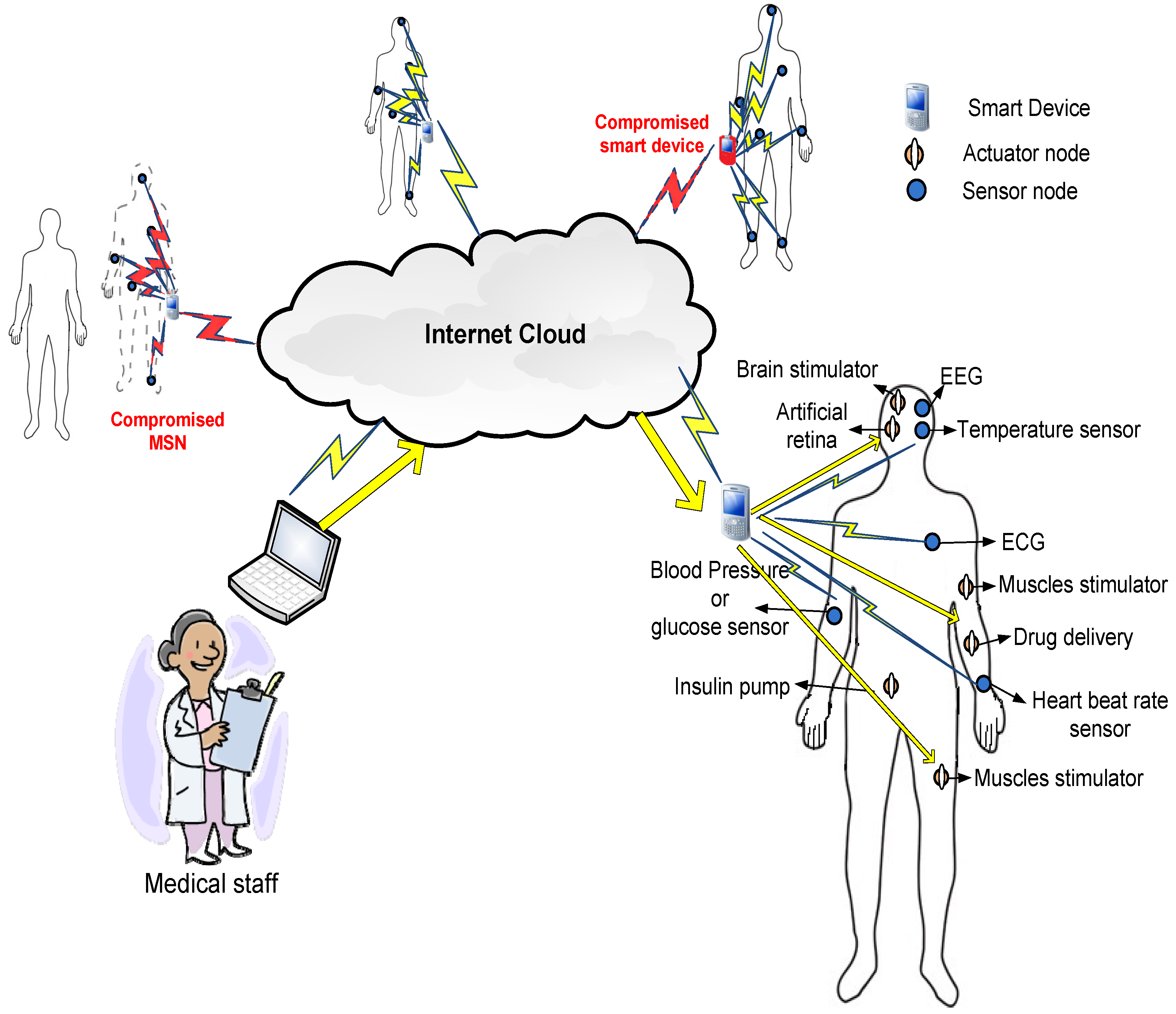
Figure 1 shows the architecture of remote patient monitoring through the MSN system that we use to demonstrate the security protocol suggested in this paper. In
Figure 1, each patient is represented as an MSN with tiny sensors or actuators reporting measurements or performing subtle actions. The MSN nodes are classified into two main types. The first type is sensor nodes that report data regularly to the smart device about the health vital signs, e.g., heart beat rate, temperature, blood pressure,
etc. [
2]. The second type is actuators that receive commands from the medical staff to perform actions and handle potential health problems, e.g., insulin pumps in the case of diabetes [
16].
There are two main security concerns in MSN architectures. The first issue is to guarantee the authenticity and integrity of the commands issued by the medical staff to the MSN actuators. The commands involve actions that are performed by the MSN nodes and may have serious impacts on the human body. Hence, masquerading as a command or creating a fake one is considered a serious threat to human life. The second issue is to ensure the confidentiality of the reported data from the MSN sensors to the medical staff.
Researchers have argued that the security protocols proposed for traditional wireless sensor networks (WSNs) and mobile
ad hoc networks (MANETs) are not directly suitable for MSNs [
17]. MSNs have unique and challenging operational and security requirements, in particular being lightweight and having low delay. For instance, protocols that use complicated and computationally-expensive cryptography (e.g., elliptic curve [
17,
18,
19,
20]) are vulnerable to denial of service (DoS) attacks where the adversary can continuously flood the MSN nodes with fake commands that may exhaust their resources and preoccupy them with verifying fake commands.
In this paper, we address the aforementioned security concerns using a lightweight public-key security protocol. This paper builds on and extends our work in Hayajneh
et al. [
1]. In particular, compared to [
1], in this paper, we added a new Related Work Section in which we discuss and compare our work with other work in the literature. We have added a Threat Model Section in the paper that discusses the adversarial model, which takes into account the adversaries’ types and their power, in addition to the possible/plausible attacks that are performed by those adversaries. Our system incorporates three parties, namely the medical staff, the smart device and the MSN nodes (which implicitly represent the patient), and in this paper, we have added the details of the security protocol (
Figure 2). The FPGA Implementation Section (FPGA stands for Field Programmable Gate Array) has been revised and expanded in this paper, where we added diagrams for the protocol design and the FPGA design flow, and also, we updated the results in
Table 1. We compare our FPGA design with other designs in the literature. Moreover, we added an Experimental Testing Section in which we implement the protocol using the Multiprecision Integer and Rational Arithmetic C/C++(MIRACL) Cryptography library. We have also compared the Rabin to Rivest, Shamir, and Adleman ( RSA) public-key cryptosystem for different key sizes; the new results are summarized in
Table 2. We have also expanded the Results and Comparisons Section and added a Security Analysis Section, which discusses the security properties of the proposed protocol.
The proposed protocol is based on the modified Rabin authentication algorithm, which has an extremely fast verification process compared to other public-key protocols. In fact, Rabin’s scheme was shown to be several hundreds of times faster and lighter than RSA [
21,
22]. The encryption that is performed by the MSN sensors is identical to the verification process. This implies that the MSN nodes are only required to perform the lightweight part of the Rabin algorithm. On the other hand, the heavy part of the Rabin scheme,
i.e., signature generation and data decryption, is performed by the medical staff or the smart device in some cases. In this paper, we modified the Rabin scheme to run components of the signature generation algorithm in parallel. This enhances Rabin scheme performance and makes it more suitable for MSN sensitive applications by reducing the potential response time.
Unlike the work in [
23,
24], in this paper, we do not focus on the user (medical staff in our case) authentication using a smart card or biometric authentication techniques. Moreover, most previous studies have assumed a well-behaved smart device that connects the MSN nodes via the Internet/cloud, a condition that might not be met in many cases. The researchers in [
17,
25,
26,
27,
28] proposed efficient remote authentication protocols for MSNs. However, they assumed that the smart device is trustworthy and did not address the issues of having misbehaving smart devices or malicious MSN nodes. A smart device is usually a smart phone that is vulnerable to malware or a malicious application. The fact that G DATA Software (a specialist company in internet security and pioneer in the field of virus protection) security experts identified 440,267 new Android malware samples in the first quarter of 2015 [
29] further supports our argument. Our authentication protocol addresses the issue of a compromised smart device efficiently by exchanging the signature between the medical staff and the MSN nodes, which is not shared with the smart device.
To evaluate the performance of the Rabin algorithm with the MSN, we implemented the algorithm with different hardware settings using the Tmote Sky mote. Moreover, the Rabin algorithm with and without the parallel settings is also implemented on an FPGA to evaluate its design and performance. Furthermore, the proposed protocol is implemented and tested using the MIRACL library. The aim is to prove that a lightweight public key can achieve the desired real-time response in cloud-based MSNs with high security and minimal power consumption.
The remainder of this paper is structured as follows.
Section 2 discusses the related work in the literature.
Section 3 presents the system and security modes, including the threat model. In
Section 4, the Rabin algorithm is described.
Section 5 illustrates the FPGA implementation where the experimental testing is presented in
Section 6.
Section 7 shows the testbed implementation.
Section 8 presents the security analysis. Finally,
Section 9 concludes the paper.
2. Related Work
In this section, an overview of the related work found in the literature regarding the security in MSN is presented. A light weight authentication scheme called TinyZKP is proposed in [
30], which is based on zero proof knowledge. However, the proposed protocol targets sensor networks where the authentication protocol authenticates the sender sensor node. A scheme to capture data confidentiality in the cloud-assisted MSNs was proposed in [
31]. Their goal was to achieve secure data communication between the cloud and MSNs without considering authentication and data integrity. He
et al. proposed a lightweight trust management protocol for sensor networks in [
32]. The proposed protocol was tested in a network of TelosB motes and was shown to improve the network performance and to protect it from malicious behaviors. A hybrid and secure priority-guaranteed MAC protocol for MSNs was proposed in [
33]. The proposed protocol used a set of security keys to prevent unauthorized access to network resources.
The authors in [
34] proposed a practical lightweight biometric approach to authenticate messages in MSN. They also developed an energy-efficient key agreement scheme that allows key sharing between MSN nodes with low overhead. Another light weight authentication protocol is found in [
35]. The authors proposed a protocol that does not depend on prior trust among the nodes by exploiting physical layer characteristics unique to an MSN. Particularly, they utilized the distinct received signal strength (RSS) variation behaviors between an on-body communication channel and an off-body channel in the authentication process, which cannot be easily forged by attackers.
For key exchange and management in MSNs, Li
et al. in [
36] proposed a group device pairing (GDP) protocol, which is an authenticated key management protocol to construct the initial trust between the MSN devices and to distribute the secret keys between them. The work in [
37] presented a Physiological Signal-based Key Agreement (PSKA) that allows neighboring nodes in an MSN to agree to a symmetric cryptographic key, in an authenticated manner, using physiological signals obtained from the human body.
The researchers in [
25,
26,
27,
28] proposed efficient remote authentication protocols for MSNs. However, they assumed that the smart device is trustworthy and did not address the issues of having a misbehaving smart device or malicious MSN nodes. Traditional public key cryptography algorithms are argued to be impractical in sensor networks because of the large computation and energy resources they require. In [
38], they showed that it is possible to design public key encryption architectures with a power consumption of less that 20
μW. They compared two architectures, the Rabin scheme and NTRUEncrypt. They showed that the Rabin scheme has no significant disadvantages compared to NTRUEncrypt.
In [
39], the researchers showed that computing a 1024-bit RSA digital signature on an eight-bit sensor node requires on the order of 90 s and 10 s for signature verification. Moreover, [
18] used signature-based Elliptic Curve Cryptography (ECC) on an eight-bit sensor node generating a 160-bit signature requiring on the order of 20 s, and 40 s are required for the verification. Moreover, In [
40], the researchers proposed a symmetric key distribution and management scheme that is based on ECC for MSNs. They reported that ECC key agreement takes about 7.2 s on a Tmote Sky mote. According to the MSN requirements, this does not satisfy the delay constraints for MSNs and makes them vulnerable to DoS attacks [
17]. The researchers in [
19,
20] reported similar results for elliptic curve Diffie–Hellman with a Tmote Sky mote.
A lightweight identity-based cryptography was presented by [
41] to balance security and privacy with accessibility for MSNs. The researchers in [
17] showed that [
41] has several security weaknesses and efficiency problems, including node replication attacks, injection of false medical data and using the computationally-extensive ECC. The researchers in [
42] proposed an ECC-based mutual authentication and access control protocol for MSNs. However, the study in [
43] identified security flaws in [
42] and showed that the scheme is susceptible to information leakage attacks. The work in [
44] presented an efficient and adaptive mutual authentication framework for real heterogeneous WSN-based applications. It is also worth mentioning that MSNs are also vulnerable to attacks that cannot be prevented using cryptographic protocols, such as: jamming [
45], packet dropping [
46,
47], wormholes [
48,
49] and localization [
50,
51].
In [
17], they proposed a lightweight system to secure wireless medical sensor networks. The proposed system was built using symmetric cryptography and hash operation. Similar to other security protocols for MSN, [
17] secure the communication between the user and the controller (smart device) and not all the way to the biosensor nodes. The work in [
52] presented an efficient anonymous authentication scheme for wireless body area networks. The protocol was based on ECC and used identity-based authentication.
In [
31], they proposed a scheme to capture data confidentiality in the cloud-assisted wireless body area networks. The goal is to achieve secure data communication between the cloud and MSNs. A secure patient-centric personal health information sharing and access control scheme in cloud computing is proposed in [
53]. The proposed scheme was proven to resist various possible attacks and malicious behaviors. In [
54], they proposed an MSN-cloud architecture to monitor a variety of biomedical conditions and to fulfill security goals for various medical services. In [
55], they proposed a hybrid authentication and key establishment scheme for MSNs. The scheme uses symmetric cryptography in sensor/actuator modes.
In summary, our work is different from previous work that assumes a trustworthy smart device and only authenticates the commands between the medical staff and the smart device (e.g., [
25,
26,
27,
28]). Our protocol secures the commands all the way to the sensors, and a compromised smart device will not have the authority to forge or modify a command. Previous work that uses computationally-expensive cryptography (e.g., [
19,
20,
40]) may exhaust the sensors limited resources and is vulnerable to DoS attacks. Our protocol is proven to be lightweight and is not vulnerable to these attacks. Moreover, protocols that rely only on symmetric cryptography will lack critical security properties, including non-repudiation, forward and backward secrecy,
etc.
3. System and Security Models
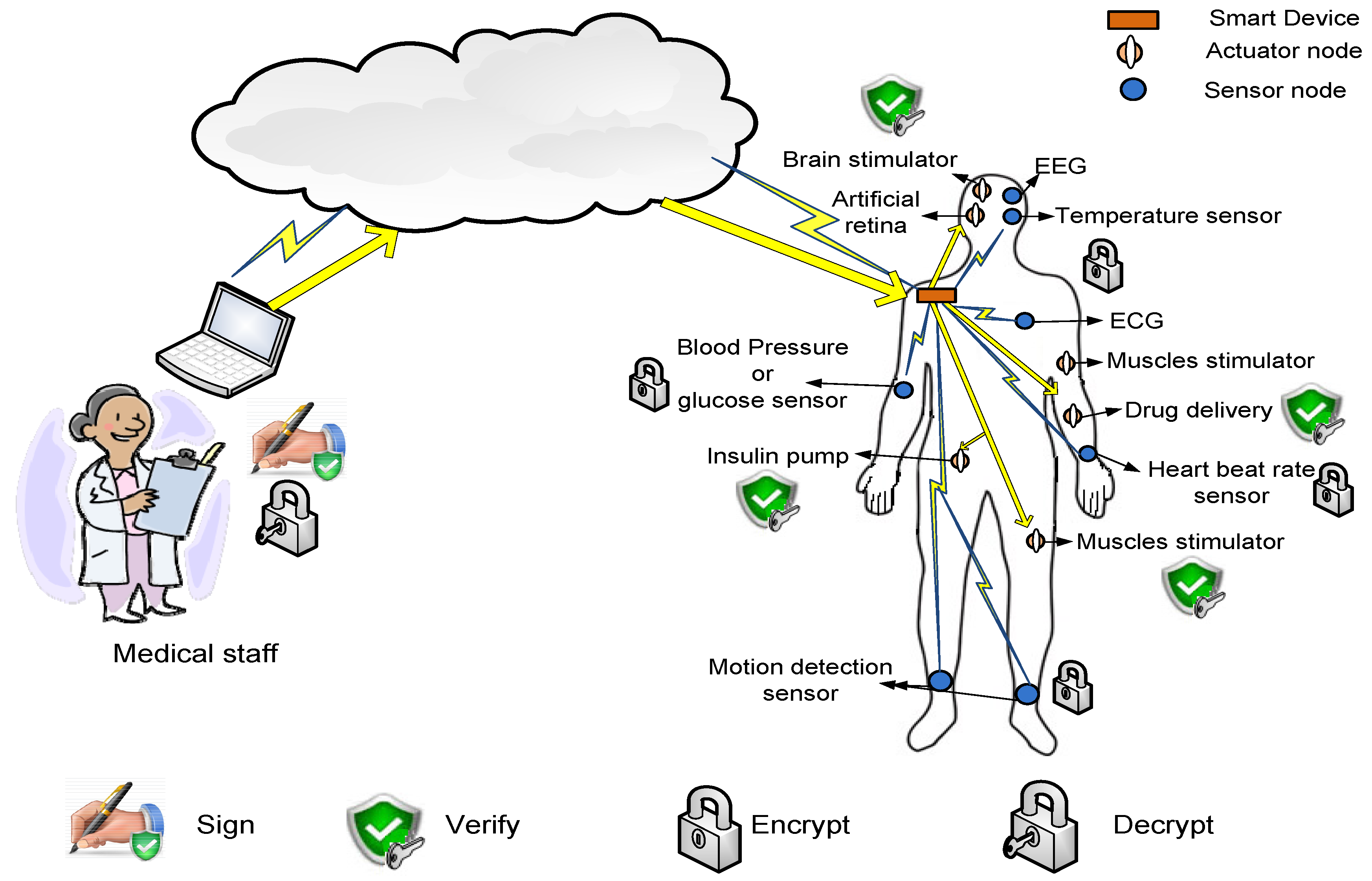
In this section, the threat, system and security models are described. In particular, the main characteristics, relations, functionalities and the basic security aspects of the smart device, the MSN nodes and the transferred data are explored. The basic MSN security architecture used in this paper is depicted in
Figure 3.
3.1. Threat Model
In this section, we introduce the threat model adopted for the proposed system. In particular, we discuss the adversarial model, which takes into account the adversaries’ types and their power, in addition to the possible/plausible attacks that are performed by those adversaries. As mentioned previously, our system incorporates three parties, namely the medical staff, the smart device and the MSN nodes (which implicitly represent the patient). These entities play different roles with respect to the threat model.
3.1.1. Adversarial Model
The adversaries (or malicious parties) in our system are classified into two categories as follows:
(1) Outsider Adversary: This category refers to any adversary who is not part of the current active communication session. In other words, the adversary is not one of the three parties in our system (i.e., medical staff, smart device, MSN nodes). We assume that all of the communications in the system take place over public channels. Thus, an outsider adversary can be a passive one who eavesdrops on the transmitted messages that are communicated between the various parties within the system or an active adversary who tries to modify the transmitted messages in a malicious way.
(2) Insider Adversary: This category includes the malicious parties within the system. As mentioned previously, the untrusted parties within the system include the smart device and the MSN nodes. However, the difference between them is related to the intended/unintended malicious behavior. Particularly, a compromised smart device is an untrusted intended party that performs any malicious behavior with the intent of harming the system. However, the MSN nodes could be both intended and unintended malicious parties in the sense that an adversary may replicate the sensor nodes and make them report invalid data to the medical staff. In this case, the MSN nodes are considered intended adversaries. On the other hand, consider the situation when the patient or the medical staff unintentionally transposes the MSN wearable sensors/actuators to a different patient from the one who is associated with these nodes in the system. In this case, the MSN nodes perform their job in an honest way all the time in terms of reporting the medical data and implementing the received medical commands; however, they are related to a different patient, and the patient profile is updated with incorrect data in the database. In this case, the MSN nodes are considered unintended adversaries.
Note that the medical staff is considered a trusted party and securely authenticated to the system; hence, all commands are being reviewed and all received information is being authenticated and checked carefully before being added to the patient profile. Moreover, in our threat model, we deal with probabilistic polynomial time (PPT) adversaries that are limited in their computational power and time.
3.1.2. Potential Attacks
We consider the following attacks in our system:
Impersonation: an adversary who tries to send fake commands or pretends to be the MSN nodes and sends invalid data to the medical staff to trigger them to issue urgent medical commands.
Commands tampering: an adversary who modifies an issued command by the medical staff and tampers with its content.
Commands replay attack: an adversary resends an old command over and over again to make the MSN nodes implement the same command multiple times.
Patient’s privacy violation attack: an adversary who collects information about the current health status of the patient.
DoS attack: an adversary who tries to disrupt system operation by sending fake commands that will consume the MSN node resources and disrupt them from performing legitimate commands.
Operation delay attack: this attack is concerned with the real-time operation of the system, where an adversary holds the command/reported data for a while and then allows them to be sent to their ultimate destination; thus, a late valid command is not useful and affects the patient’s health in a negative way, especially in urgent situations.
Note that in all pf the above attacks, the intended adversary can be either an outsider adversary who listens to the communication channel and tries to carry out the attacks or a malicious smart device that is considered an intermediary between the MSN nodes and the medical staff and, thus, has the privilege of watching the entire traffic within the system. However, for the unintended adversary, we have the impersonation attack, where the MSN nodes are placed on a different patient from the one registered by the medical staff. Thus, they are reporting correct data about the body that does not match the correct patient profile.
3.2. System Model
In our system, we assume two types of smart devices: relay and smart master nodes. In the first type, the smart device collects the reported data from the MSN nodes, reports them to the medical staff, receives commands from the medical staff and sends them back to the intended MSN nodes. In the second type, the smart device has additional functionality to process the reported data from the MSN nodes and to generate suitable commands to handle a potential health problem faced by the patient. We do not recommend using the second type, as it assumes a trusted smart device, which is not a valid assumption, as elaborated earlier. In the first type, the smart device could be a regular MSN node, i.e., it has limited hardware, software and power capabilities; while in the second one, it could be portable smart digital devices in which the computational and power resources are abundant.
The MSN nodes used in our system, as shown in
Figure 3, are also classified into two types: sensors and actuators. The sensors are able to monitor the body health indicators and to generate data packets of the measured data. Examples of MSN sensors include sensors to measure the body temperature, the heart beat rate, the blood pressure, ECG, EEG,
etc. [
2,
56]. On the other hand, the actuators are nodes that have the suitable hardware to perform actions specified by the commands sent by the medical staff at the cloud side or the smart device. Examples of MSN actuators are: artificial retina, insulin pump, automatic drug delivery, muscles stimulator,
etc. [
16]. Both MSN sensors and actuators complement each others’ work,
i.e., based on the reported data by the sensors, the needed action is performed by the actuators.
Moreover, as illustrated in
Figure 3, the data transmitted through the network is also divided into two types: periodic reported data by the sensors and commands generated by the medical staff/smart devices. The periodic data are sent on a regular basis with different packet sizes based on the sensor type. For example, ECG sensors send large data packets and more frequently than temperature sensors [
56]. For the commands, their frequency depends on the health status of the patients. Patients with critical situations may receive more commands compared to patients with stable body health signs.
3.3. Security Model
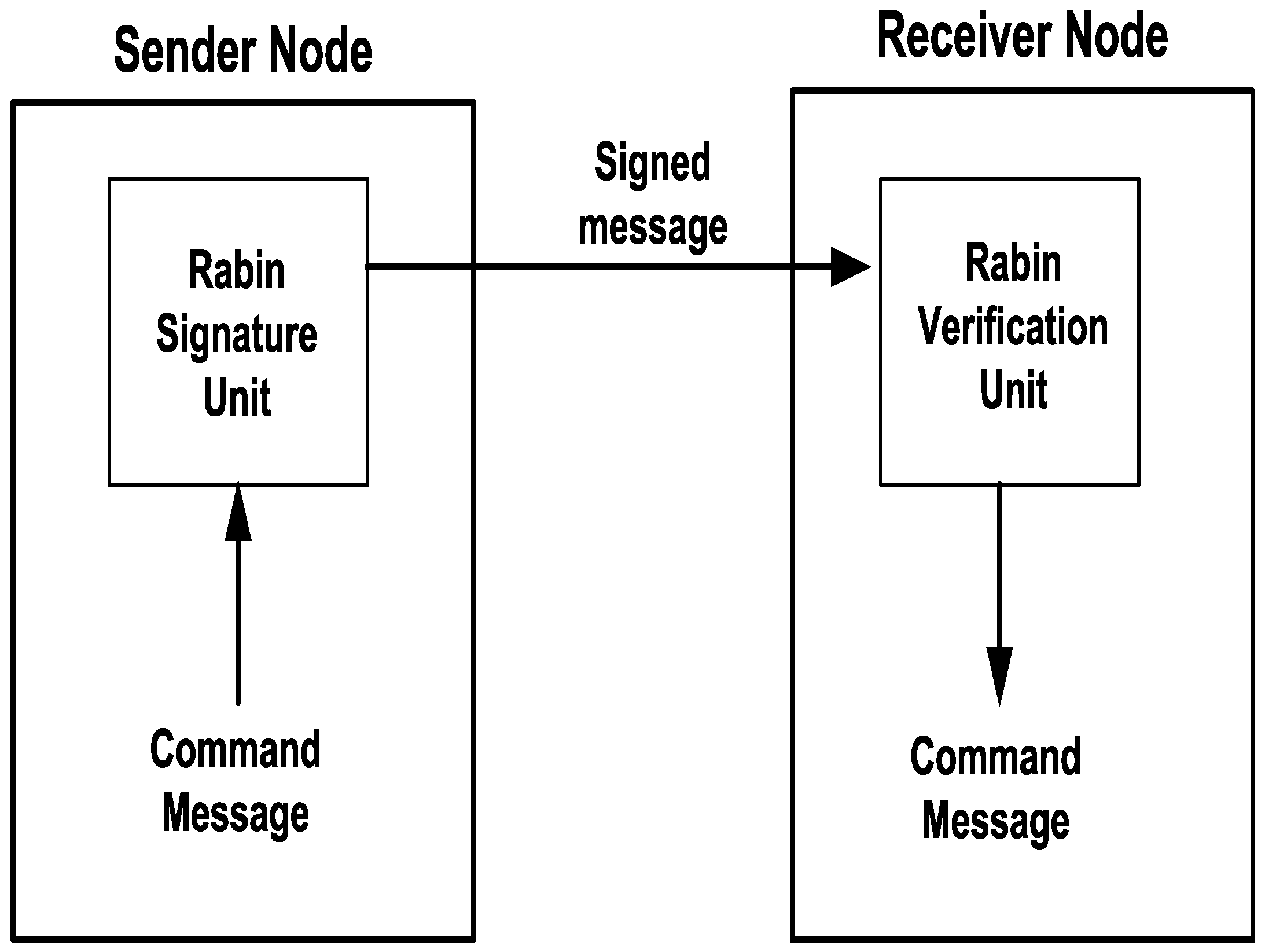
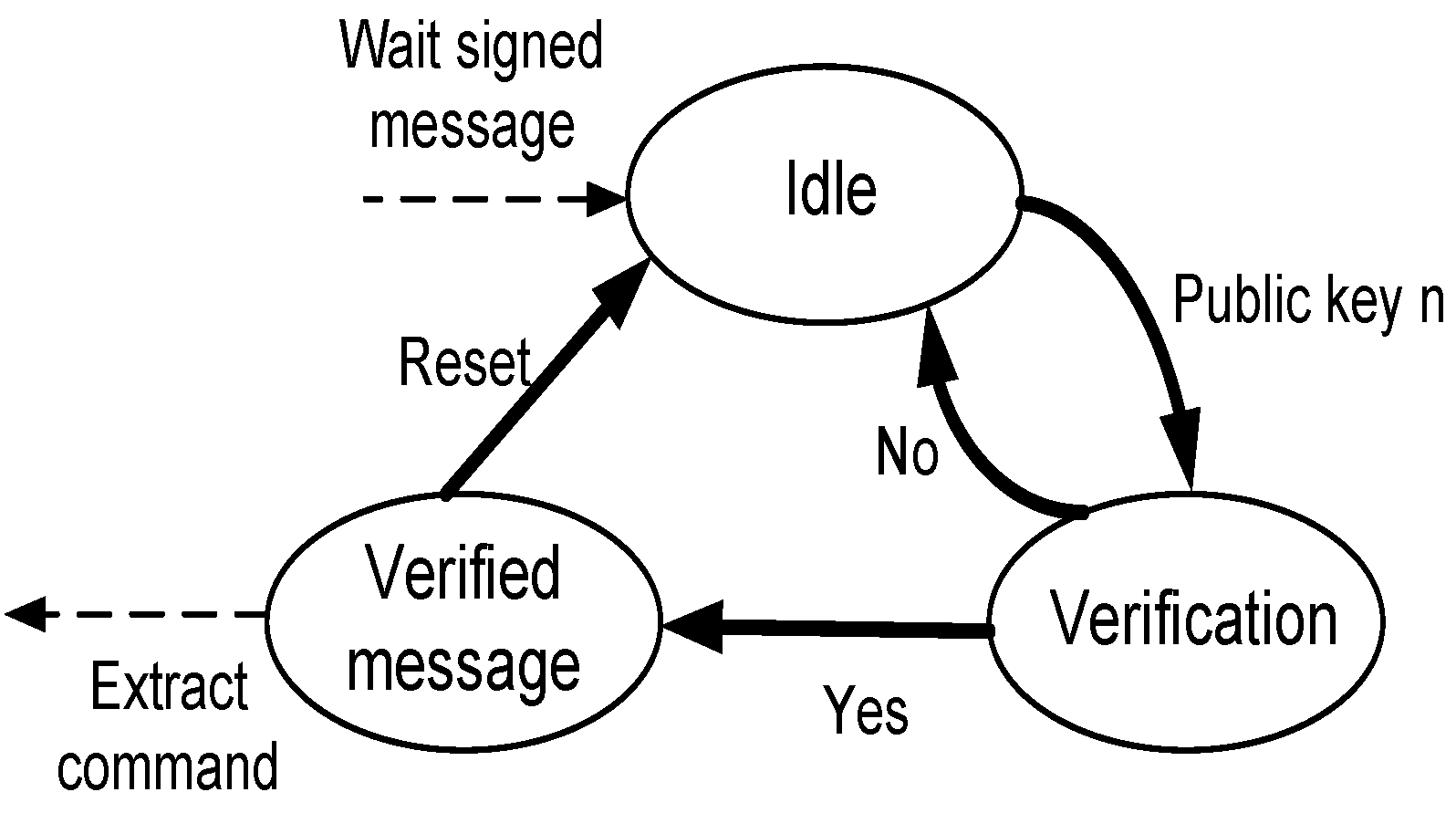
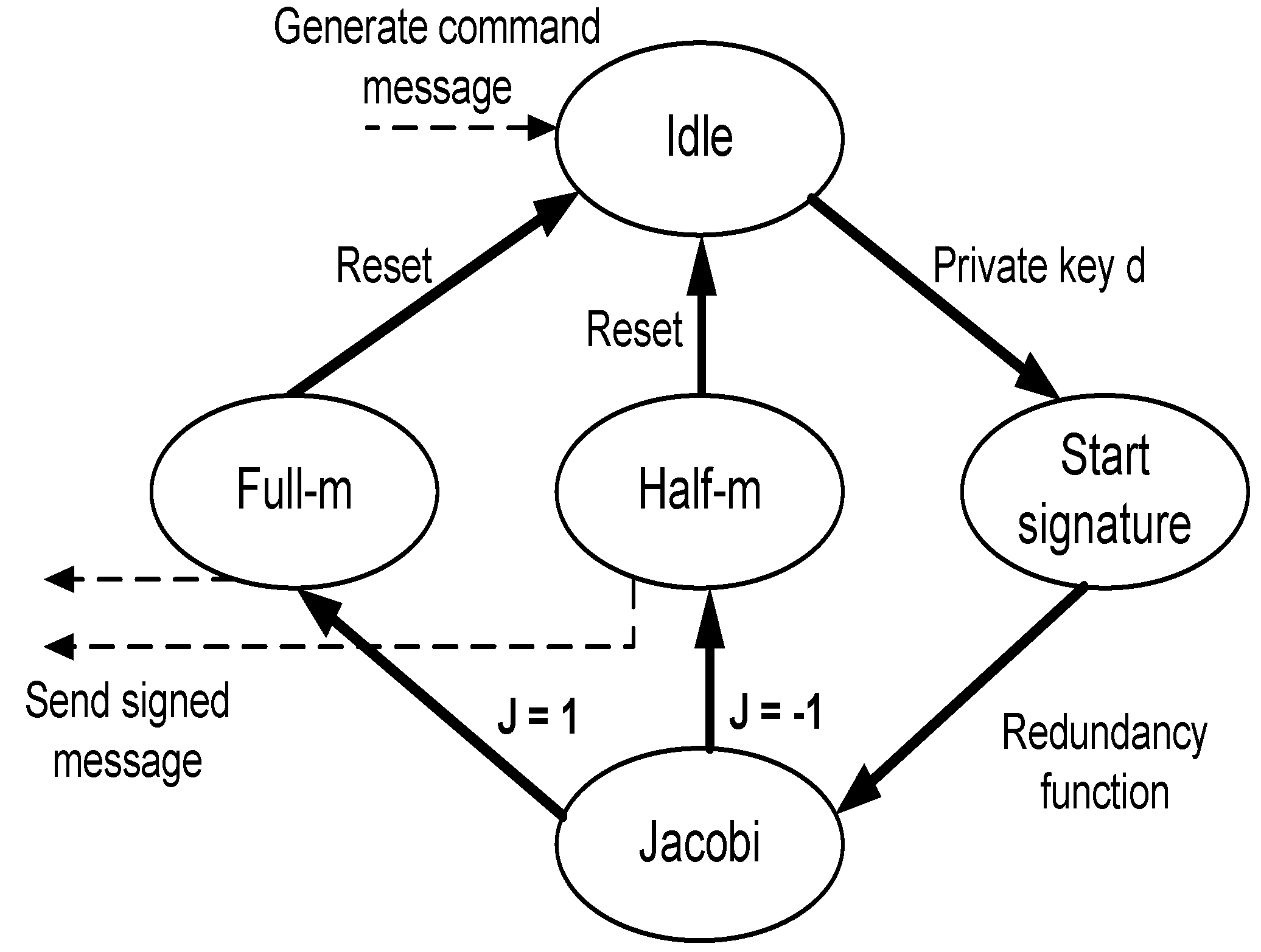
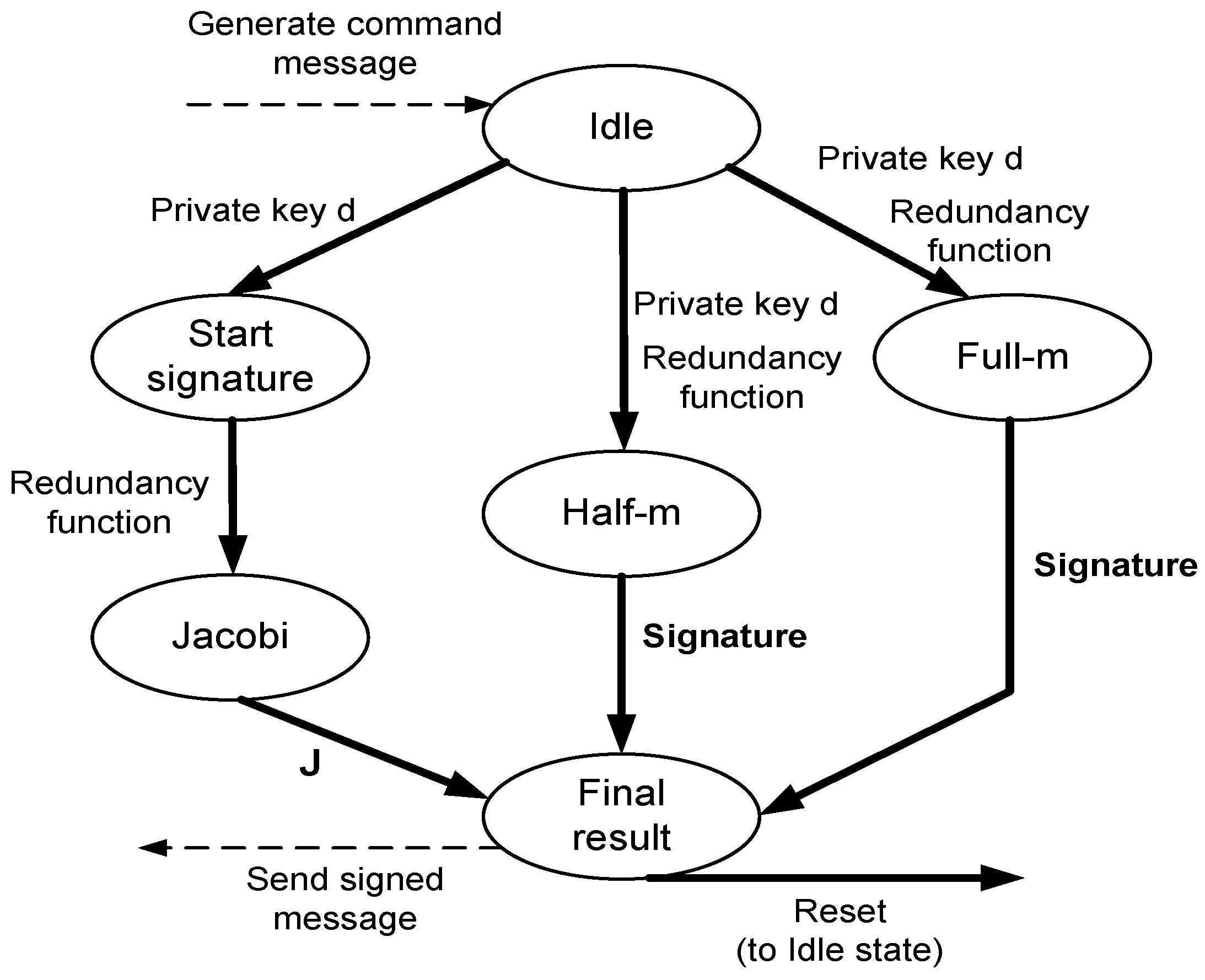
The details of the proposed security protocol are presented in
Figure 2. The medical staff generates a command and nonce using a random number and time stamp. The command is encrypted using any symmetric key cipher, and a digital signature is generated for the command combined with the nonce. The smart device only forwards the command and the digital signature to the MSN node, which will verify the digital signature and use the nonce to verify the freshness of the command and detect a replay attack. As for encrypting the sensor-reported data, we suggest two options for this process. The first option is to use Rabin encryption; the sensors in this case will use the public key of the medical staff to encrypt the data with some secret concatenated with the data to prevent an attacker from sending fake data. The send option is to simple use symmetric cryptography with the same key that the medical staff used to encrypt the command. It is also worth noting that the Rabin encryption is identical to the signature verification, while Rabin decryption is identical to signature generation.
As elaborated earlier, one of the most critical security issues in the presented remote patient monitoring system with MSNs is to guarantee that the commands issued by the medical staff, usually located at the cloud side, to the actuators are not altered or fake. Due to the large number of MSN nodes, their wide distribution and the possibility for insertion/removal of MSN nodes, we argue that using public-key cryptography is the most efficient solution to achieve the desired security requirements. The MSN nodes need only to store the public key(s) of the medical staff that are authorized to issue controlling commands. Although being a less computationally-expensive option, using symmetric cryptography imposes new challenges in terms of key management and distribution. However, if a computationally-expensive public-key cryptographic system is used to provide all security services, then it will burden the MSN nodes and result in long delays and energy consumption.
Since the main security process that MSN nodes perform is to verify the authenticity of a signed message, we decided to use a public-key scheme that has a fast and efficient signature verification process. We found that the Rabin algorithm is an excellent candidate that satisfies our requirements [
57]. The medical staff or smart device signs their issued commands using a digital signature with their private key. Then, the MSN nodes use the medical staff or smart device public key to verify the integrity and authenticity of the delivered commands.
Another important security service that can also be covered by our proposed security framework is the confidentiality of the reported data from the sensors to the medical staff. In this case, the MSN nodes encrypt their reported data using the medical staff or smart device public key. Fortunately, with the Rabin scheme, this process is identical to the verification process and is considered extremely light compared to the verification process of other public key algorithms.
A possible variation of the proposed protocol is to use the public key cryptography only to exchange authentication and encryption keys securely. The keys should be only exchanged between the medical staff and the sensors, which keep the smart device outside the loop. In this case, the protocol can be based on symmetric cryptography, which is lighter than asymmetric cryptography. It is critical in this case to generate and exchange new authentication and encryption keys each time the medical staff wants to communicate with sensors to ensure that the system satisfies the security properties that will be discussed in
Section 8.
6. Experimental Testing
The MIRACL Cryptography library [
74] has been used in the experimental testing. It supports the needed building blocks of the designed protocol in addition to big number arithmetic, which are required in public key cryptographic-based protocols. In addition, this library is known to be significantly fast and is widely used to implement applications for embedded systems and low power devices, which makes it a good fit for MSN nodes. However, MIRACL does not include several protocols that are required in this paper, such as the Rabin, RSA and hashed message authentication code (HMAC) . Hence, we have coded these protocols and added them to MIRACL.
6.1. Protocol Implementation and Results
As for the implementation, the following parameter values were used: a modulus size of 1024 bits for the public key schemes and a medical command of size 40 bytes. The strong random generator (SRNG) in MIRACL has been used to generate random primes p and q randomly. This SRNG as described in the library documentation is proven to generate random numbers suitable for cryptographic applications. It needs both a strong seed and a random string of a size of 256 bytes to be initialized. For the seed, we have used the /dev/random utility in Linux to get truly randomly-generated seeds. For the random text, either the same utility can be used to get a highly random string or any random keystroke sequence from the keyboard can be read.
As for the key generation, for RSA, the public key exponent is selected first where different values have been tested to see the effect on the algorithm operation. Based on the selected value, then strong random primes are generated. For the Rabin algorithm, the strong random primes are generated while ensuring the basic keys properties, i.e., (mod8) and (mod8).
For RSA, PKCS1.5 has been used to pad the sent messages where a 16-byte random number is added in front of the message. For the decryption, the Chinese remainder theorem has been used to speed up the decryption process. As for the hash function, it was implemented using SHA-3. Finally, the Rabin scheme for digital signature generation and verification has been implemented as described earlier in the paper.
After the system has been initialized and all needed keys are generated, the medical staff may generate a command that needs to be delivered to the MSN actuator. Both the command and the digital signatures are then generated and sent to the smart device, which will simply forward that to the MSN nodes, as shown in
Figure 2. The protocol implementation has been debugged and checked for the result correctness of the generated keys, the encryption and decryption process and digital signature generation and verification.
All programs were tested on the same machine, and we are interested in the computational speed of the different protocol parts. We provide results for the process speed of the signature verification and generation. This is due to the fact that our target is to find a digital signature scheme that is fast to verify to support the real-time response of the system without consuming the nodes’ computational resources and power. The protocol has been tested using the following machine specifications: a laptop with core i7, 8 GB RAM and Ubuntu 12.04 operating system. The proposed protocol has been tested under different scenarios or key sizes: the first one denoted as Rabin uses this algorithm for the digital signature, and the other three modes all apply RSA with different key sizes: RSA-128 with a 128 key size, RSA-256 with a 256 key size, RSA-512 with a 512 key size and RSA-1024 with a 1024 key size.
The results found in
Table 2 prove the objective of the proposed protocol, that is using the Rabin algorithm for the digital signature is much faster in the verification than RSA. As shown in the table, Rabin outperformed all RSA versions, including the low-power exponent RSA, where it achieves the least computational delay. Thus, the MSN nodes are able to verify the signature in a fast way, and so, the command will be executed faster to handle the patient’s health situation. In addition, the Rabin signature generation speed is comparable to RSA modes. However, this process is performed by the medical staff, which is not limited in resources, and it can be equipped with more powerful hardware components to speed up this operation; as opposed to the MSN actuators, which are limited in their resources and should have a small size to enable the construction of the MSN network. In addition, it is noted that as the key size in RSA is increased, the total delay of the medical staff operation is reduced. This is due to the fact that as the public key is larger, this means that the private key is smaller, and so, the signature generation process will be faster; this is verified by the results found in
Table 2, which depict the speed of the signature generation and verification processes.
7. Testbed Implementation
In this section, we explore the testbed implementation used to evaluate the performance of the proposed security model. Similar to [
75,
76], we used TinyOS and the nesC language to develop the algorithms code and to upload them on Moteiv Tmote sky motes. In what follows, the main aspects of the tools used, the implementation details, the experiments’ setup and the obtained results are discussed.
7.1. Implementation Tools and Setup
TinyOS is an open-source operating system designed for wireless embedded sensor networks. It features a component-based architecture, which enables rapid innovation and implementation while minimizing the code size, as required by the severe memory constraints inherent in sensor networks. The TinyOS component library includes network protocols, distributed services, sensor drivers and data acquisition tools. nesC is an extension to the C language designed to embody the structuring concepts and execution model of TinyOS. To develop the code of the signature and verification algorithms, we translated the big number library from C to nesC. The translated library allows mathematical operations of numbers of a size of 512 bits.
Tmote sky is an ultra low power wireless module that can be used in rapid application prototyping. Tmote leverages industry standards like USB and IEEE 802.15.4 to interoperate seamlessly with other devices. It uses an 8-MHz Texas Instruments MSP430 microcontroller with 10 k RAM and 48 k flash. Although Tmote is one of the advanced customizable sensor nodes, its computational capabilities remain very limited, and this constraint must be considered while building the intended MSNs.
The packet format used in TinyOS is the same one used in 802.15.4. The default data field has a maximum size of 29 bytes. We created our own structure to use the data field of the packet as illustrated in
Table 5.
The src field is the source address of the sending mote; pID is the ID of the current packet (used for fragmentation); Offset is the offset from the initial packet (used for fragmentation); message is the message to be sent; and finally, signature is the signature generated by the medical staff/smart device. As shown, the first three fields are of a size of one byte, while the message is of a size of four bytes, and the signature field has a size of 20 bytes. In our experiments, the commands signature is of a size of 64 byte; hence, we need four packets for each signature to be sent. To enable us to view the packets sent by the motes, we ran the Serial Forwarder on the ComPort of the mote and the Listener tool available in TinyOS.
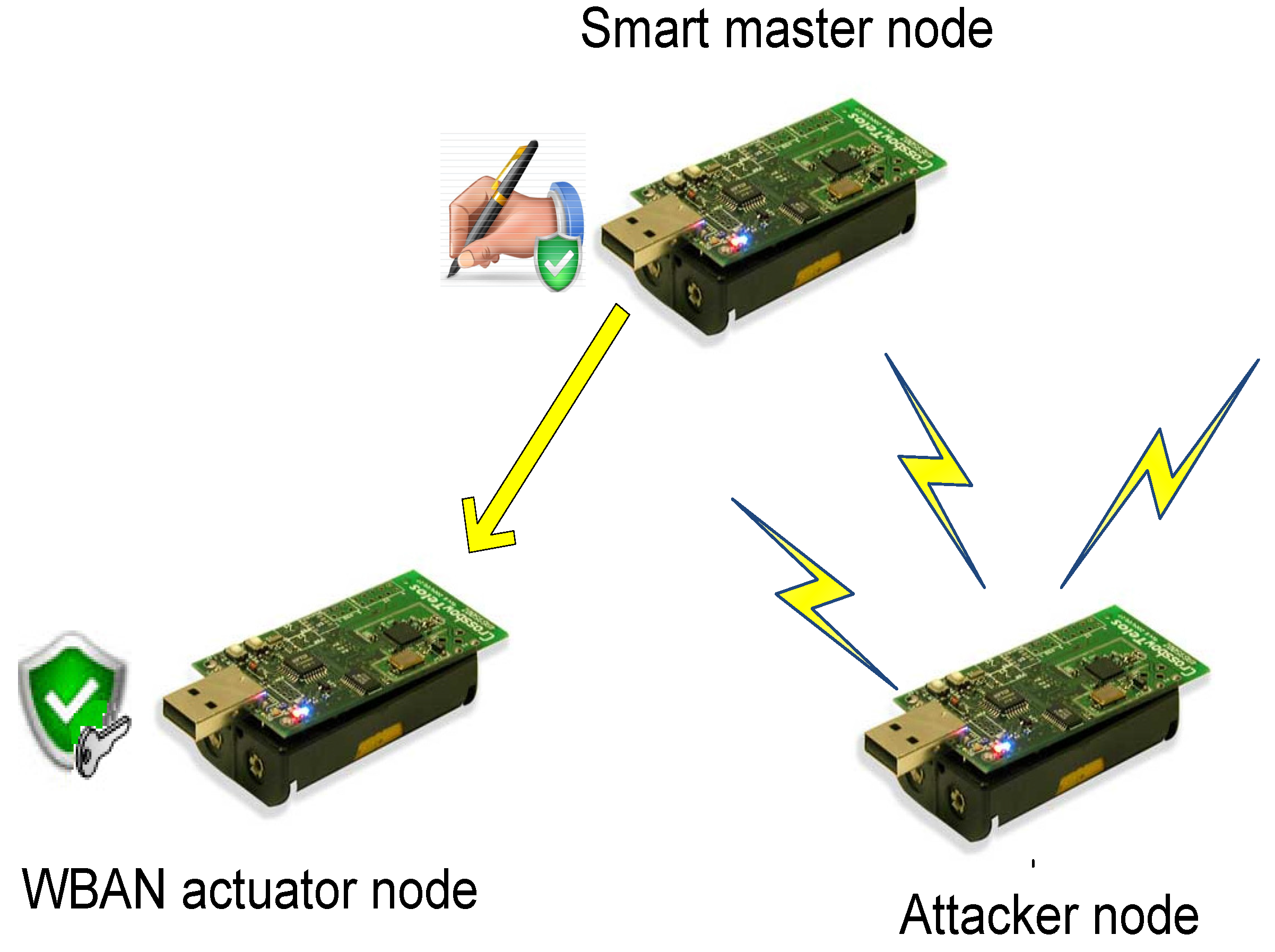
7.2. Experiment Setup
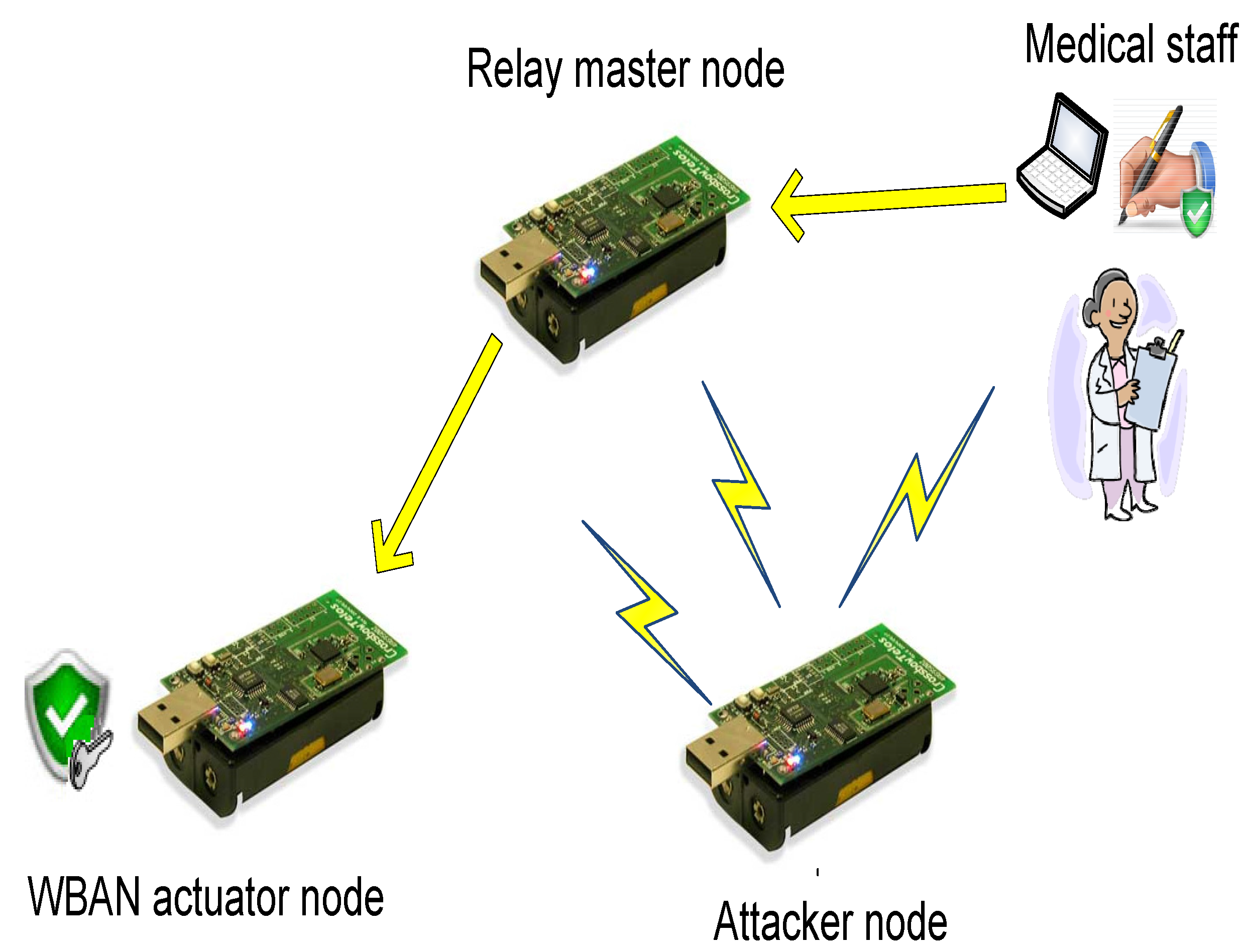
We built a testbed that contains three motes: the smart device node, the MSN node and an attacker node. The testbed has been configured to depict two different scenarios. In the first one, shown in
Figure 10, the relay smart device is tested. However, in the second scenario, the same mote is configured to mimic the smart mote functionality that generates signed commands; see
Figure 11.
The MSN node is the receiver mote that runs the verification algorithm. Two of the LEDs found on the Tmote sky are used to indicate whether the verification is successful or not as follows: the green LED turns ON if the signature is verified, and the red LED turns ON if the verification of the signature fails. The third blue LED can also be used to indicate that the node is sending or receiving data.
The relay smart device node is a mote running TOSBase, which is an application in TinyOS that makes the mote act as a bridge between the serial device (a PC) and the radio link (our wireless network). This application includes queues in both directions to guarantee that once a message enters the queue, it eventually leaves on the other interface. On the mote, this can be visually observed for every packet received and successfully bridged by the toggling of the green LED.
The smart device mote uses its own public/private key pair and runs the signing algorithm to generate the signature. We programmed the smart device mote to send the signature in four fragments, where one fragment is sent every 400 ms. The receiver mote collects these fragments in a global variable, putting each piece in its correct position. Once it receives all four fragments, it runs the verification algorithm and indicates the result on the LEDs, as mentioned before. Finally, we programmed the attack mote to impersonate the smart device and to send a bogus signature to the receiver mote.
7.3. Results and Comparisons
As mentioned earlier, we used big numbers of a size of 512 bits for all variables used by the signature and all intermediate calculation. Generally, public key authentication incorporates complex computations, which results in slow performance and high power consumption. Therefore, we evaluated the proposed security model in terms of the needed operations and time to sign/verify the commands.
In terms of computational requirements, the Rabin scheme has only one expensive operation on the receiver mote, which is squaring the received signature modulo the public key. Note that this operation is much less expensive than the two expensive operations that are performed during the generation of the signature, i.e., computing the Jacobi symbol (which is a recursive function that uses modulo), and the modular exponentiation. However, this is a concern for the smart device node that is an MSN node (limited hardware resources). If the medical staff is performing the command signing process, the signing complexity is not an issue where high power devices are used for processing. However, in this case, achieving a rapid response with minimal delay is still desirable.
We note that the security of our algorithm relies on the problem of factoring a large integer. Similar to breaking the RSA, Rabin’s scheme is broken under a chosen-message attack. More specifically, if an attacker can choose two messages and obtain their signatures from our signing motes, the signature of the product of the two messages will be the product of the two signatures of the original messages.
The above attack could be harmful for sensor networks in two ways. First the attacker can use it to mount a denial of service attack on a certain mote. This is because using a valid message and signature pair, he or she can force the mote to compute the verification algorithm, therefore consuming its resources and causing a delay in processing other legitimate messages. On the other hand, construction of a message from the product of two messages could allow a prudent attacker to obtain a message that he or she can use to trick the receiver into believing the received message is reasonable. For example, in a fire monitoring application, which relies on temperature readings, an attacker can add the two temperatures, causing the receiver to trigger a false alarm.
For the second scenario with the smart device node, we obtained a signature generation time average of 22 s. The verification time on the other hand took less than 1 s. This result is very encouraging, as it reduces the computational requirements on the receiver to verify an incoming signature. It also reduces the effect of a DoS attack in the case of a malicious node sending bogus signatures or packets. On the other hand, using the parallel settings proposed in the previous section, the average signature generation time was reduced to 5 s.
We note that these signing and verification times are much lower than what can be achieved using other public key authentication protocols. In [
39], the researchers showed that computing a 1024-bit RSA digital signature on and eight-bit sensor node requires on the order of 90 s and 10 s for signature verification. Moreover, [
18] used signature-based Elliptic Curve Cryptography (ECC) on an eight-bit sensor node generating a 160-bit signature requiring on the order of 20 s and around 40 s for the verification.
Table 6 compares the signature generation and verification timing for different schemes.
As for the energy consumption, in [
38], they showed that it is possible to design public key encryption architectures with a power consumption of less that 20
μW. They compared two architectures, the Rabin scheme and NTRUEncrypt, and the results showed that the Rabin scheme has no significant disadvantages compared to NTRUEncrypt. The latter is close to being practical on sensor nodes.
However, SNEP (Secure Network Encryption Protocol) and
μ TESLA (Timed, Efficient, Streaming, Loss-tolerant Authentication Protocol) [
77] used only symmetric key-based techniques to provide security. The main problem is that they require each node to be time synchronized with the base station and require key management functions and ample storage. This also causes a delay in the authentication process and might not be practical for real-time sensitive MSN applications. Further, the Merkle-Winternitz signature [
78] used efficient one-time signature constructions that are computed quickly on sensor networks. Their problem is that they require high communication overhead on the order of 100–200 bytes per signature. Finally, in [
79], they used a one-way hash function to conduct public key authentication in sensor networks. They assumed that they can exchange the one-way hash values of their public key securely prior to the deployment. Their results claimed an 86% energy savings compared to public key authentication.
Our public key approach differs from existing symmetric key approaches in that it only assumes the existence of public-key infrastructure (PKI) (or that the public/private keys are pre-installed authentically on the sensors). Moreover, there is no need for key establishment/management or re-keying.
Finally, the Rabin algorithm offers advantages compared to
μ TESLA.
μ TESLA is a broadcast authentication protocol, which is a lighter, efficient version of TESLA, and it is suitable for resource-constrained sensor networks [
77]. Compared to
μ TESLA, our scheme does not require time synchronization or any initialization messages to be sent. Moreover,
μ TESLA requires the receiver to wait a predetermined amount of time, usually a few time slots, before starting the verification process of the received messages. In the Rabin scheme, receivers start verification immediately after receiving the commands, where the entire process takes around 1 s, making it suitable for real time applications.


 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}