
An Open Platform for Seamless Sensor Support in Healthcare for the Internet of Things


 ,
,
Abstract
:1. Introduction
1.1. Related Work
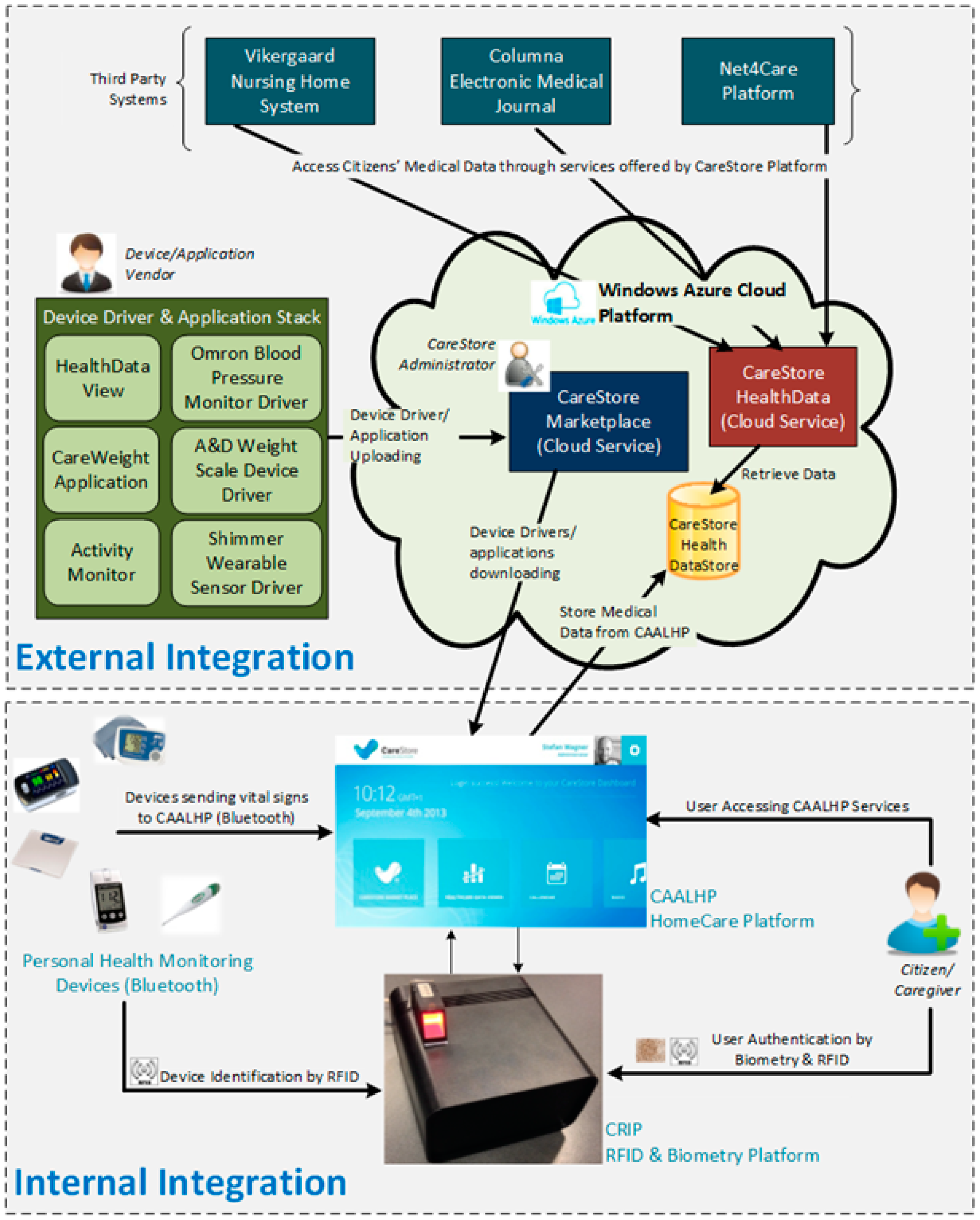
1.2. The CareStore Platform
- CAALHP: The Common Ambient Assisted Living Home Platform is an open-source runtime execution platform for execution of services, applications, device drivers and a user interface (UI) for staff and residents interaction with the platform;
- CRIP: Common Recognition and Identification Platform used to identify staff, residents and devices, using RFID and/or biometrics as identification technologies;
- CareStore Marketplace: An online shared platform for uploading and storing healthcare and AAL drivers and applications, that can be downloaded and installed in a seamless way on the CAALHP and the CRIP.
2. Materials and Methods
2.1. Requirements
- Integration: The CRIP subsystem shall provide a seamless integration with internal and external subsystems. A standard interface for easy access by other subsystems shall be provided. The major integration is made with CAALHP, which has the ability to communicate with the CareStore Marketplace in order to download device drivers/profiles and applications;
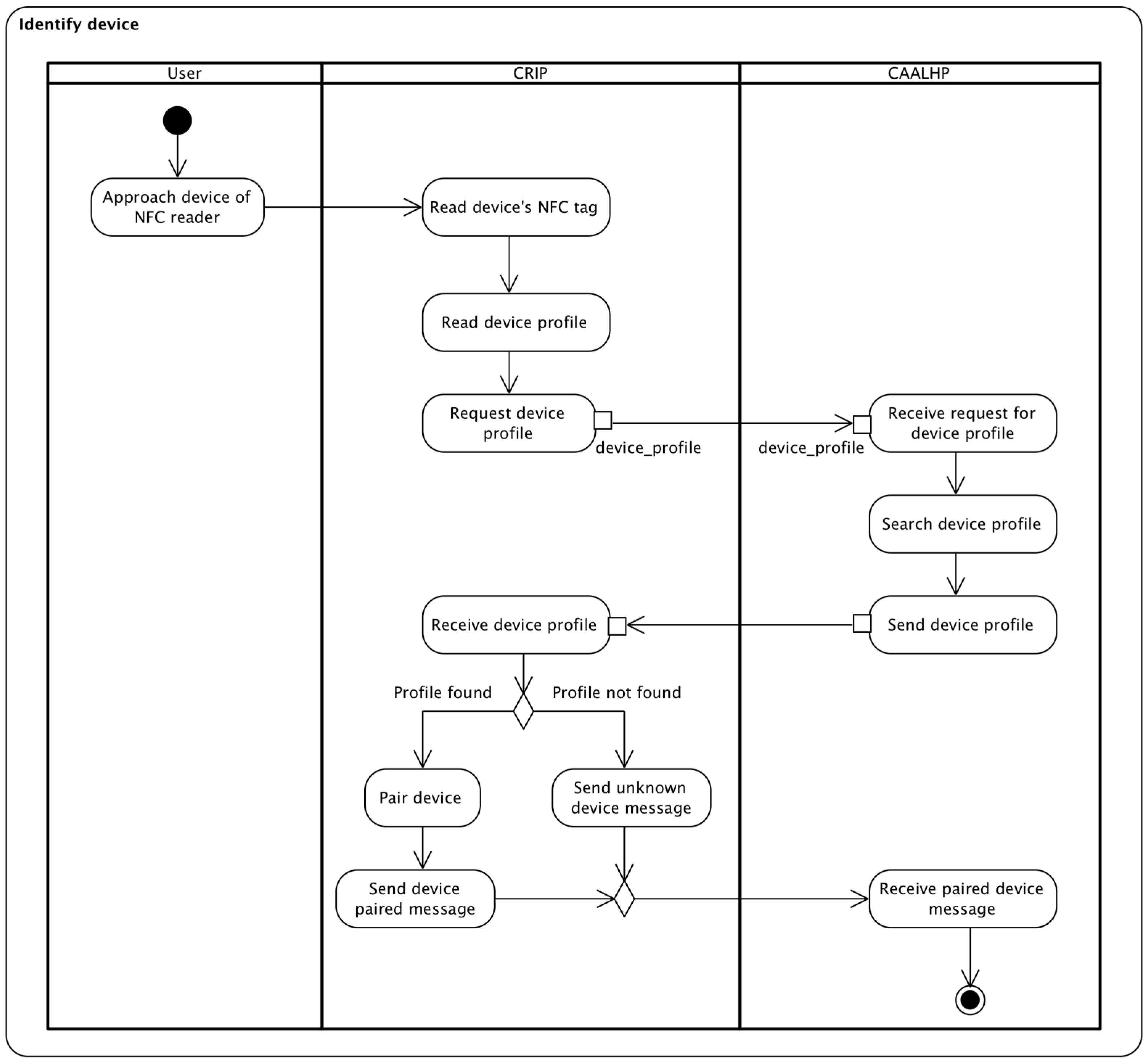
- Device Installation and Configuration: The device installation and configuration shall be absolutely seamless and shall involve minimal interaction with the end-user. A CareStore user must initiate the identification of devices by approaching a device with a NFC tag of the NFC reader. After identification is over, the user is notified via CAALHP that a new device is available;
- Locking during installation process: When a device is being installed, the user shall still be able to use other devices or CAALHP applications, which are not part of installation process;
- Failure notifications: The system shall provide a timely response in case of errors and report the failure events. For example, when an application fails to install or integrate with a health device then the end-user and administrator users shall be notified simultaneously. The notification shall also be sent if an application or device fails to respond or crashes during use or execution.
- Citizen: A system’s user under care either on a private home or in a nursing home, who can use the homecare platform. A Citizen can seamlessly add a new device by holding it close to the homecare platform and have it install any necessary device drivers and automatically configure them for use;
- Caregiver: Can be a doctor, nurse or relative of the Citizen who provides medical treatment to him. Caregivers can add new wireless health devices in a similar way as a Citizen;
- CAALHP: Part of the homecare platform that allows integration of different assisted living technologies, making it easier to operate and deploy new AAL and telemedicine devices and applications. CAALHP is connected with CRIP, in order to perform authentication and retrieve data from the personal health devices;
- Device: Represents a dedicated personal health device, which is used for monitoring inhabitants in an AAL scenario.
- The users must register on the platform before they can perform any action on it. For now, this registration process must be made with the presence of another authorized user (e.g., a caregiver). The registration process includes registering the user’s fingerprint and creating an NFC card that can be used for future identification. A combination of fingerprint and card for authentication might only be required for highly secure actions;
- The users’ biometric credentials may be stored locally on the CRIP, for those who are allowed on a particular homecare deployment. This will provide better performance, because the CRIP will be able to authenticate users from the local CAALHP “user profiles” storing authorized users;
- The communications among different subsystems of the CareStore platform must be encrypted and signed to ensure data security. In particular, the health data of citizens is security-sensitive and it is important to secure it during communication.
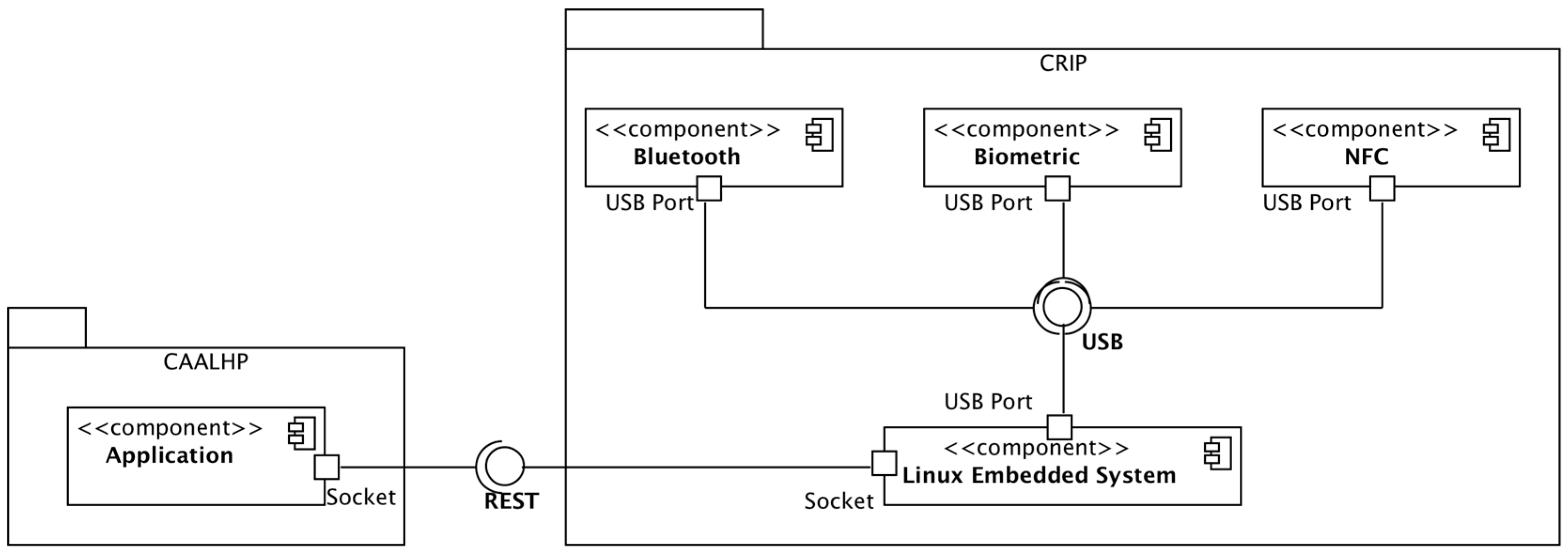
2.2. Hardware Architecture
- Bluetooth: Bluegiga BT111 [40] is a low cost and ultra-small BLE module designed for applications where both Bluetooth Classic and BLE connectivity are needed. The module already includes the USB interface and the antenna. It is capable of detecting devices within a range of 100 m and it is compatible with Linux and the BlueZ Bluetooth stack;
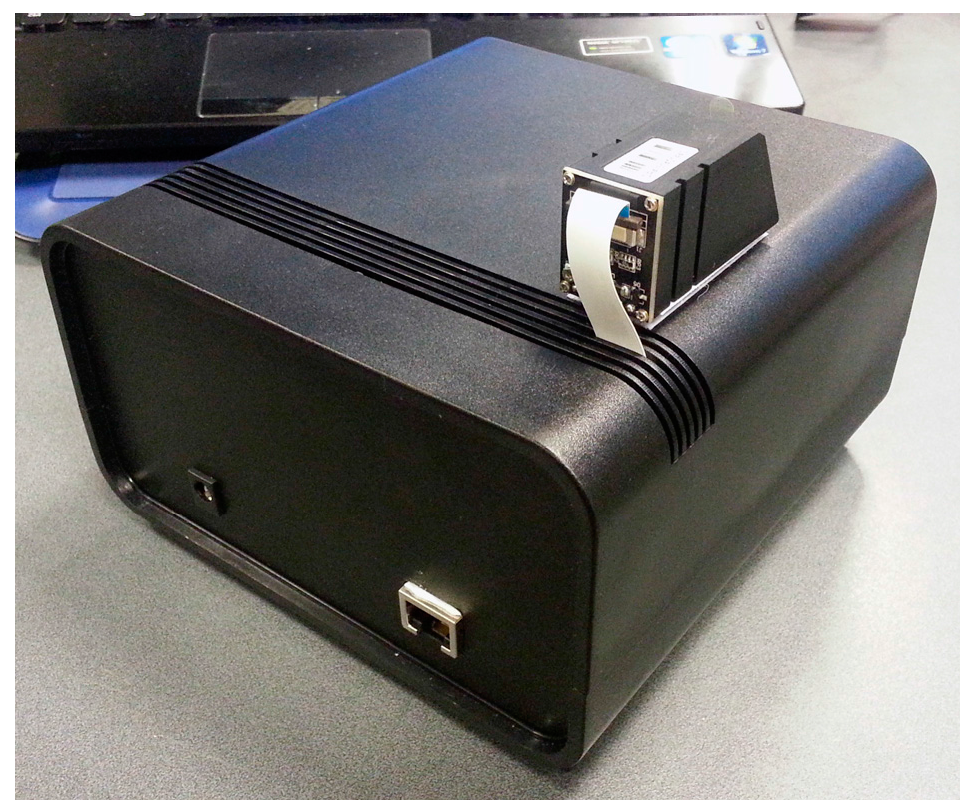
- Biometric Module: Suprema Inc.’s SFM3520-OP [41] is an embedded module with a rugged optical fingerprint sensor with a high quality fingerprint image for both dry and wet fingers. It comes with a reliable and fast fingerprint analysis algorithm (matching speed of 1:1 in 800 ms and 1:N in 970 ms) and internal memory that can save up to 9000 fingerprint templates. Although it does not support USB natively, the serial communication can be retrofitted with USB by using appropriate conversion hardware;
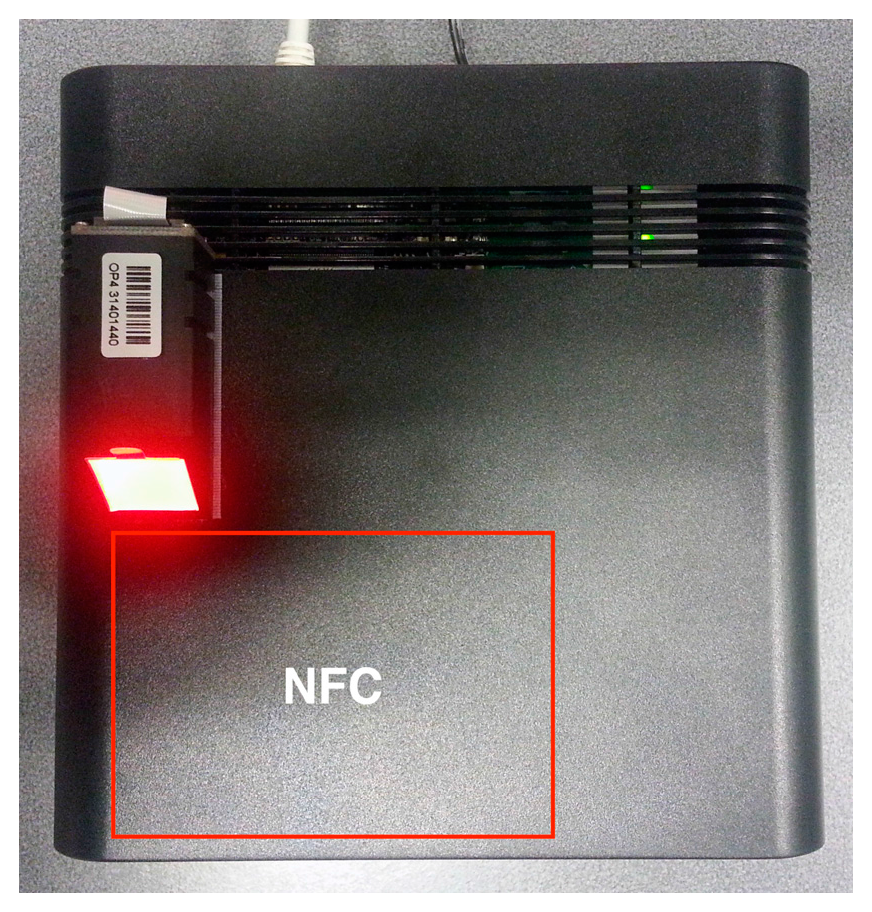
- NFC Module: The Advanced Card Systems ACR122 [42] is a RFID proximity card that supports the Mifare, ISO 14443 A and B, and FeliCa NFC technologies. It is possible to connect it by USB and the operating distance is up to 5 cm, depending on the type of card and/or proximity tags;
- Embedded Linux Platform: Our choice was the Raspberry Pi [43] due to its wide availability and community support. Other platforms were evaluated, namely the Kontron M2M [44] and the Intel Galileo (Gen 1) [45], but they were discarded because of: (1) higher price than the Raspberry Pi, and (2) less support, with the Galileo having, at the time, minimal support due to its early market release, while on the Kontron it was more complex to create and manage Linux images.
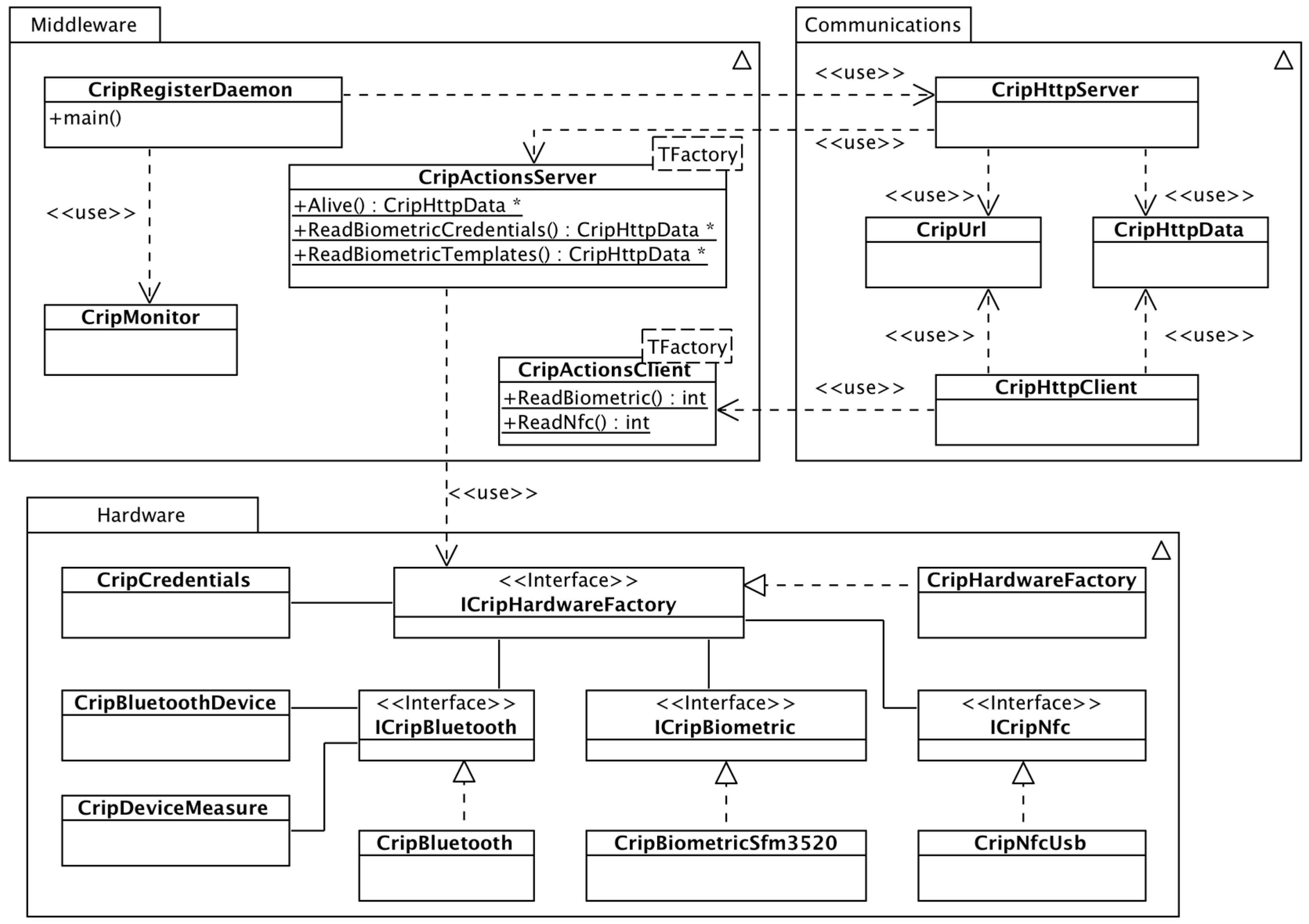
2.3. Software Architecture
2.3.1. Module Middleware
2.3.2. Module Communications
2.3.3. Module Hardware
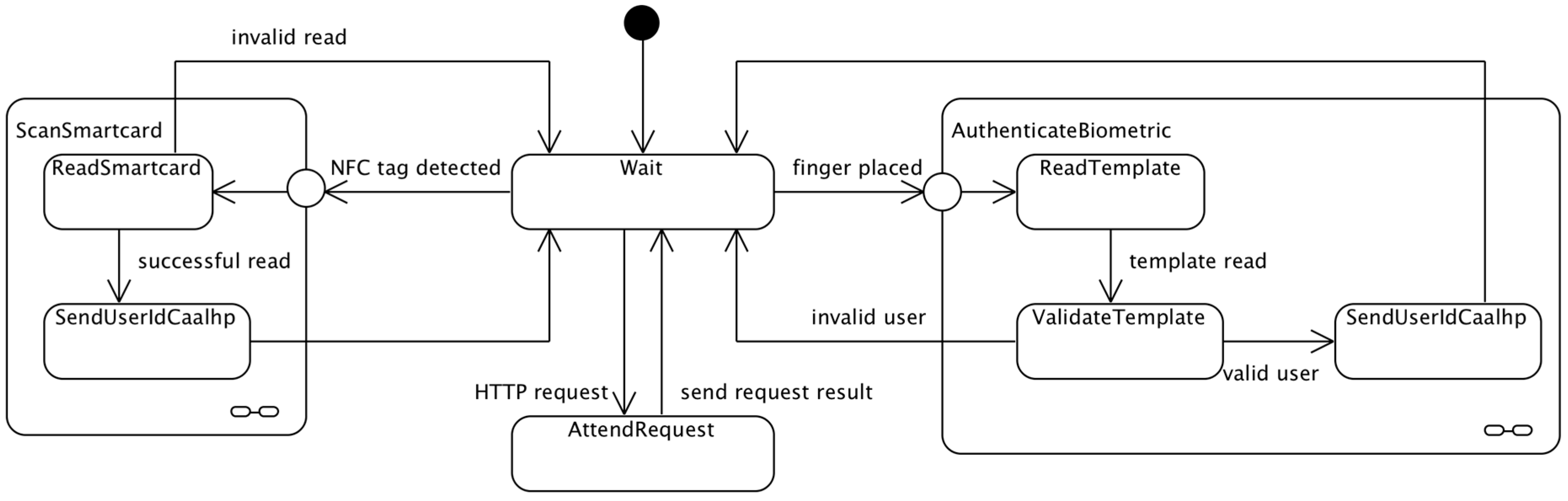
2.3.4. Software States Overview
2.3.5. Bluetooth Pairing Using NFC
2.4. Evaluation Protocols
2.4.1. CRIP’s Test Application
- (1)
- “Read biometric templates” allows reading user fingerprint templates from the biometric hardware, so they can later be stored. For each user, two biometric templates are read to improve fingerprint recognition due to finger placement;
- (2)
- “Store templates” allows storing user’s templates collected in option 1. The templates are stored on the biometric hardware and a user is recognized once he tries to authenticate at any moment;
- (3)
- “Scan for Bluetooth devices” performs a scan for Bluetooth devices near CRIP. This option is used mainly for development and test purposes;
- (4)
- “Write UID on NFC card” writes the user’s UID data on a NFC tag;
- (5)
- “Write Bluetooth data on NFC tag” writes the Bluetooth device’s information on a NFC tag that can later be used to identify and pair a Bluetooth device;
- (6)
- “Write device data on NFC tag” writes custom information regarding a non-Bluetooth device on a NFC tag, so that the device can be identified by the CRIP;
- (7)
- “Check CRIP status” sends an alive message to CRIP to check its current status.
2.4.2. Protocol for Users’ Identification
2.4.3. Protocol for Devices Identification and Communication
3. Results
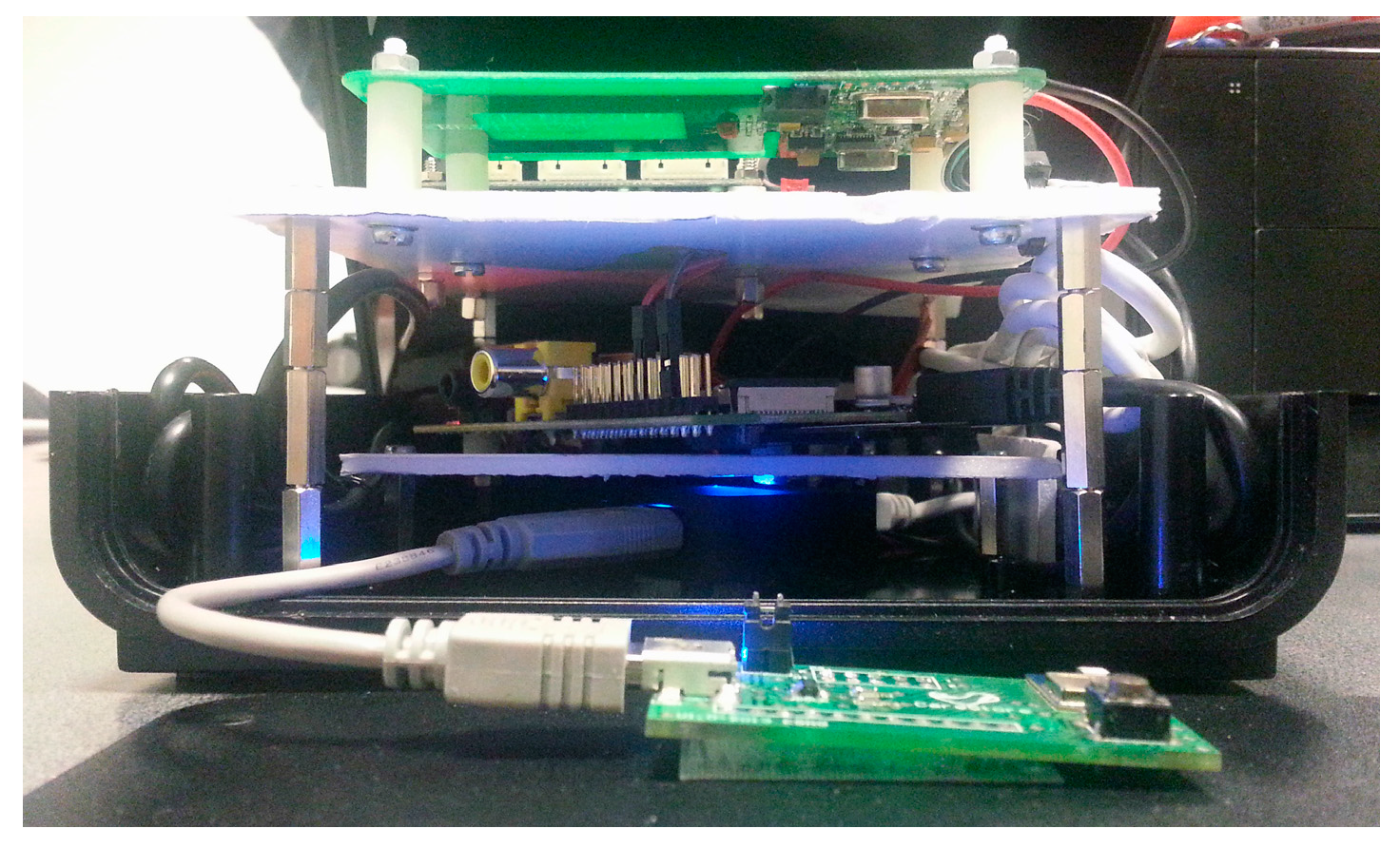
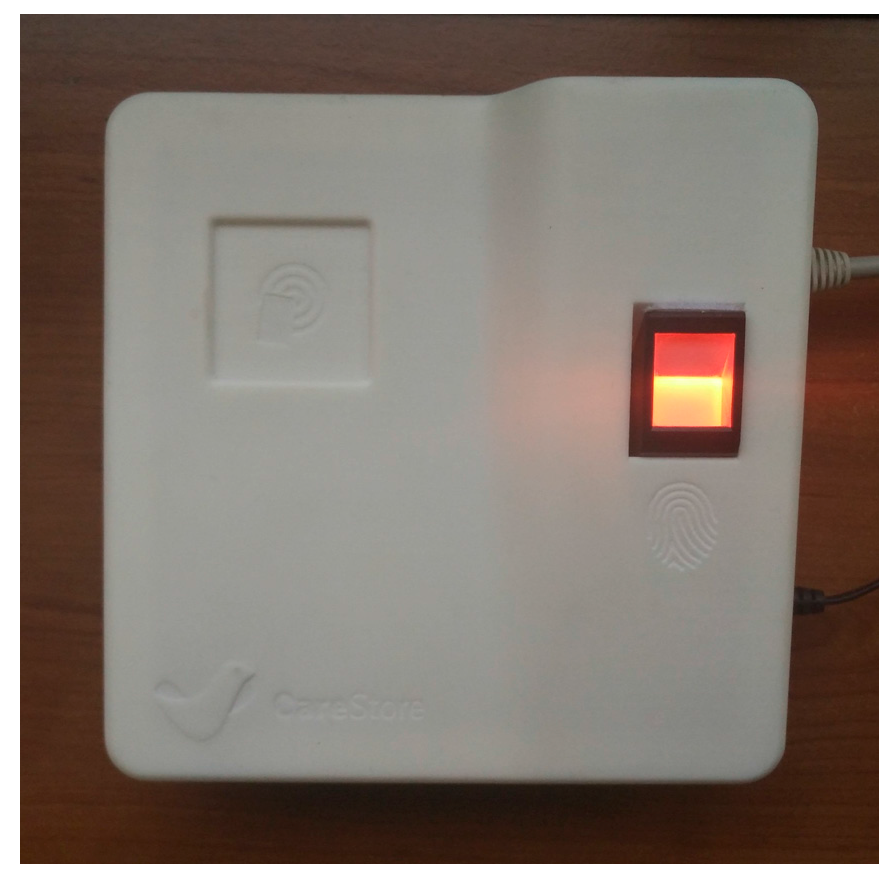
3.1. CRIP Prototypes
- A Raspberry Pi Model B+ was used, instead of the previous Model B. This model started to be commercialized during the project’s development and was adopted because the Model B would be discontinued. Also, the dimensions and connections of the board allow a more compact design;
- The Bluetooth module is now integrated on the same board as the biometric module. This option was chosen to reduce the hardware size;
- A new custom power and USB hub board was developed. The power part provides 5 V from the main power supply to all hardware peripherals of the system, enhancing the voltage and current stabilization on all boards. The USB hub circuit is similar to the Conceptronic USB hub used on the first prototype. Our option to keep using it was mainly based on the need to eliminate possible powering issues of the first prototype, which was successfully done. All peripherals were connected to the hub and this was connected to the Raspberry Pi through USB;
- The operating system was stored on a USB pen drive, while on the first prototype was on a SD card. This option was made due to the flash memory architecture used by a pen drive, which offers better resilience against file system corruption in case of failure such as a power outage. Still, a SD card was needed for booting the Raspberry Pi’s Linux.
3.2. Users Identification and Authentication
3.3. Health Devices Identification and Communication
4. Discussion
4.1. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European Commission. The 2015 Ageing Report; European Commission: Brussels, Belgium, 2015. [Google Scholar]
- Kroezen, M.; Dussault, G.; Craveiro, I.; Dieleman, M.; Jansen, C.; Buchan, J.; Barriball, L.; Rafferty, A.M.; Bremner, J.; Sermeus, W. Recruitment and retention of health professionals across Europe: A literature review and multiple case study research. Health Policy 2015, 119, 1517–1528. [Google Scholar] [CrossRef] [PubMed]
- Scheil-Adlung, X. Extension of Social Security Long-Term Care Protection for Older Persons: A Review of Coverage Deficits in 46 Countries; International Labour Office: Geneva, Switzerland, 2015. [Google Scholar]
- Organisation for Economic Cooperation and Development (OECD). How’s Life? 2015; OECD Publishing: Paris, France, 2015. [Google Scholar]
- World Health Organization (WHO). Targets and Beyond—Reaching New Frontiers in Evidence; The European Health Report 2015; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Bardram, J.E. Pervasive healthcare as a scientific discipline. Methods Inf. Med. 2008, 47, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, H.; Magaireah, A.I. Factors affecting the adoption of integrated cloudbased e-health record in healthcare organizations: A case study of Jordan. In Proceedings of the 6th International Conference on Information Technology and Multimedia, Putrajaya, Malaysia, 18–20 November 2014; pp. 102–107.
- Bernocchi, P.; Scalvini, S.; Bertacchini, F.; Rivadossi, F.; Muiesan, M.L. Home based telemedicine intervention for patients with uncontrolled hypertension—A real life non-randomized study. BMC Med. Inform. Decis. Mak. 2014, 14, 52. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Ferrari, R. The role of telemedicine in hypertension management: Focus on blood pressure telemonitoring. Curr. Hypertens. Rep. 2015, 17, 21. [Google Scholar] [CrossRef] [PubMed]
- Sieverdes, J.C.; Gregoski, M.; Patel, S.; Williamson, D.; Brunner-Jackson, B.; Rundbaken, J.; Treiber, E.; Davidson, L.; Treiber, F.A. mHealth medication and blood pressure self-management program in Hispanic hypertensives: A proof of concept trial. Smart Homecare Technol. Telehealth 2013, 1, 1–10. [Google Scholar] [CrossRef]
- Carlisle, K.; Warren, R. A qualitative case study of telehealth for in-home monitoring to support the management of type 2 diabetes. J. Telemed. Telecare 2013, 19, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Neinstein, A.; Wong, J.; Look, H.; Arbiter, B.; Quirk, K.; McCanne, S.; Sun, Y.; Blum, M.; Adi, S. A case study in open source innovation: Developing the Tidepool Platform for interoperability in type 1 diabetes management. J. Am. Med. Inform. Assoc. 2016, 23, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Neumann, C.L.; Wagner, F.; Menne, J.; Brockes, C.; Schmidt-Weitmann, S.; Rieken, E.M.; Schettler, V.; Hagenah, G.C.; Matzath, S.; Zimmerli, L.; et al. Body weight telemetry is useful to reduce interdialytic weight gain in patients with end-stage renal failure on hemodialysis. Telemed. e-Health 2013, 19, 480–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.B.; Cadmus-Bertram, L.A.; Natarajan, L.; White, M.M.; Madanat, H.; Nichols, J.F.; Ayala, G.X.; Pierce, J.P. Wearable Sensor/Device (Fitbit One) and SMS text-messaging prompts to increase physical activity in overweight and obese adults: A randomized controlled trial. Telemed. e-Health 2015, 21, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Odeh, B.; Kayyali, R.; Nabhani-Gebara, S.; Philip, N.; Robinson, P.; Wallace, C.R. Evaluation of a Telehealth Service for COPD and HF patients: Clinical outcome and patients’ perceptions. J. Telemed. Telecare 2015, 21, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Whitten, P.; Mickus, M. Home telecare for COPD/CHF patients: Outcomes and perceptions. J. Telemed. Telecare 2007, 13, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Dyrvig, A.-K.; Gerke, O.; Kidholm, K.; Vondeling, H. A cohort study following up on a randomised controlled trial of a telemedicine application in COPD patients. J. Telemed. Telecare 2015, 21, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; He, W.; Li, S. Internet of things in industries: A survey. IEEE Trans. Ind. Inform. 2014, 10, 2233–2243. [Google Scholar] [CrossRef]
- Varshney, U. Pervasive healthcare and wireless health monitoring. Mob. Netw. Appl. 2007, 12, 113–127. [Google Scholar] [CrossRef]
- Bui, N.; Zorzi, M. Health care applications: A solution based on the internet of things. In Proceedings of the 4th International Symposium on Applied Sciences in Biomedical and Communication Technologies, Barcelona, Spain, 26–29 October 2011; pp. 1–5.
- Riazul Islam, S.M.; Kwak, D.; Kabir, H.; Hossain, M.; Kwak, K.-S. The internet of things for health care: A comprehensive survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Atzori, L.; Iera, A.; Morabito, G. The Internet of Things: A survey. Comput. Netw. 2010, 54, 2787–2805. [Google Scholar] [CrossRef]
- Stankovic, J.A. Research directions for the internet of things. IEEE Internet Things J. 2014, 1, 3–9. [Google Scholar] [CrossRef]
- Aijaz, A.; Aghvami, A.H. Cognitive machine-to-machine communications for internet-of-things: A protocol stack perspective. IEEE Internet Things J. 2015, 2, 103–112. [Google Scholar] [CrossRef]
- Ko, J.; Lu, C.; Srivastava, M.B.; Stankovic, J.A.; Terzis, A.; Welsh, M. Wireless sensor networks for healthcare. Proc. IEEE 2010, 98, 1947–1960. [Google Scholar] [CrossRef]
- Amendola, S.; Lodato, R.; Manzari, S.; Occhiuzzi, C.; Marrocco, G. RFID technology for IoT-based personal healthcare in SmartSpaces. IEEE Internet Things J. 2014, 1, 144–152. [Google Scholar] [CrossRef]
- Wagner, S.; Hansen, F.O.; Pedersen, C.F.; Memon, M.; Aysha, F.H.; Mathissen, M.; Nielsen, C.; Wesby, O.L. CareStore platform for seamless deployment of ambient assisted living applications and devices. In Proceedings of the 7th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth), Venice, Italy, 5–8 May 2013; pp. 240–243.
- Memon, M.; Wagner, S.R.; Pedersen, C.F.; Beevi, F.H.A.; Hansen, F.O. Ambient assisted living healthcare frameworks, platforms, standards, and quality attributes. Sensors 2014, 14, 4312–4341. [Google Scholar] [CrossRef] [PubMed]
- Rashvand, H.F.; Salcedo, V.T.; Sánchez, E.M.; Iliescu, D. Ubiquitous wireless telemedicine. IET Commun. 2008, 2, 237–254. [Google Scholar] [CrossRef]
- Rahmani, A.M.; Thanigaivelan, N.K.; Gia, T.N.; Granados, J.; Negash, B.; Liljeberg, P.; Tenhunen, H. Smart e-health gateway: Bringing intelligence to Internet-of-Things based ubiquitous healthcare systems. In Proceedings of the 2015 12th Annual IEEE Consumer Communications and Networking Conference (CCNC), Las Vegas, NV, USA, 9–12 January 2015; pp. 826–834.
- Catarinucci, L.; de Donno, D.; Mainetti, L.; Palano, L.; Patrono, L.; Stefanizzi, M.; Tarricone, L. An IoT-aware architecture for smart healthcare systems. IEEE Internet Things J. 2015, 2, 515–526. [Google Scholar] [CrossRef]
- Cubo, J.; Nieto, A.; Pimentel, E. A cloud-based Internet of Things platform for ambient assisted living. Sensors 2014, 14, 14070–14105. [Google Scholar] [CrossRef] [PubMed]
- Saponara, S.; Donati, M.; Fanucci, L.; Celli, A. An Embedded sensing and communication platform, and a healthcare model for remote monitoring of chronic diseases. Electronics 2016, 5, 47. [Google Scholar] [CrossRef]
- Yang, G.; Xie, L.; Mantysalo, M.; Zhou, X.; Pang, Z.; Xu, L.; Kao-Walter, S.; Chen, Q.; Zheng, L. A health-IoT platform based on the integration of intelligent packaging, unobtrusive bio-sensor and intelligent medicine box. IEEE Trans. Ind. Inform. 2014, 10, 2180–2191. [Google Scholar] [CrossRef]
- Ghose, A.; Bhaumik, C.; Das, D.; Agrawal, A.K. Mobile healthcare infrastructure for home and small clinic. In Proceedings of the 2nd ACM International Workshop on Pervasive Wireless Healthcare—MobileHealth’12, Hilton Head, SC, USA, 11–14 June 2012; p. 15.
- Miranda, J.; Cabral, J.; Ravelo, B.; Wagner, S.; Pedersen, C.F.; Memon, M.; Mathiesen, M. Wireless authentication platform for healthcare applications. In Proceedings of the 2015 IEEE International Wireless Symposium (IWS 2015), Shenzhen, China, 30 March–1 April 2015; pp. 1–4.
- Miranda, J.; Cabral, J.; Ravelo, B.; Wagner, S.; Pedersen, C.; Memon, M.; Mathiesen, M. Radiated EMC immunity investigation of common recognition identification platform for medical applications. Eur. Phys. J. Appl. Phys. 2015, 69, 11002. [Google Scholar] [CrossRef]
- Wagner, S.; Beevi, F.H.A.; Pedersen, C.F.; Miranda, J.; Cabral, J.; Ravelo, B. Evaluation of Caregivers’ first time use of a seamless deployment platform. In Proceedings of the 10th EAI International Conference on Pervasive Computing Technologies for Healthcare, Cancun, Mexico, 16–19 May 2016; pp. 59–66.
- Personal Connected Health Alliance. Available online: http://www.pchalliance.org/continua/ (accessed on 14 October 2016).
- Bluegiga BT111 Bluetooth Smart Ready HCI Module. Available online: http://www.silabs.com/pro-ducts/wireless/bluetooth/bluetooth-smart-modules/Pages/bt111-bluetooth-smart-ready-hci-module.aspx (accessed on 14 October 2016).
- Suprema Inc. SFM3520-OP. Available online: http://www.supremainc.com (accessed on 14 October 2016).
- Bit4id ACR122. Available online: http://www.bit4id.com (accessed on 14 October 2016).
- M2M Smart Services Developer Kit—Kontron. Available online: http://www.kontron.com/downloads/datasheet/datasheet_m2m.pdf (accessed on 14 October 2016).
- Raspberry Pi. Available online: https://www.raspberrypi.org (accessed on 14 October 2016).
- Intel® Galileo Development Board. Available online: http://www.intel.com/content/www/us/en/embedded/products/galileo/galileo-g1-datasheet.html (accessed on 14 October 2016).
- Libmicrohttpd. Available online: https://www.gnu.org/software/libmicrohttpd (accessed on 14 October 2016).
- Libcurl. Available online: http://curl.haxx.se/libcurl/ (accessed on 14 October 2016).
- BlueZ. Available online: http://www.bluez.org (accessed on 14 October 2016).
- Antidote. Available online: http://oss.signove.com/index.php/Antidote_IEEE_11073_stack_library (accessed on 14 October 2016).
- Libnfc. Available online: http://nfc-tools.org (accessed on 14 October 2016).
- Bluetooth® Secure Simple Pairing Using NFC, Application Document. Available online: https://www.bluetooth.org/DocMan/handlers/DownloadDoc.ashx?doc_id=264234 (accessed on 14 October 2016).
- Intel Linux NFC. Available online: https://01.org/linux-nfc (accessed on 14 October 2016).
- Open NFC. Available online: http://www.open-nfc.org/ (accessed on 14 October 2016).
- A&D UA-767PBT-C—Upper Arm Blood Pressure Monitor. Available online: http://www.aandd.jp/products/medical/bluetooth/ua_767pbt_c.html (accessed on 14 October 2016).
- A&D UC-321PBT-C—Precision Health Scale. Available online: http://www.aandd.jp/products/medical/bluetooth/uc_321pbt_c.html (accessed on 14 October 2016).
- Fisher, R.; Ledwaba, L.; Hancke, G.; Kruger, C. Open hardware: A role to play in wireless sensor networks? Sensors 2015, 15, 6818–6844. [Google Scholar] [CrossRef] [PubMed]
- Medaglia, C.M.; Serbanati, A. An overview of privacy and security issues in the internet of things. In The Internet of Things; Springer: New York, NY, USA, 2010; pp. 389–395. [Google Scholar]
- Keoh, S.L.; Kumar, S.S.; Tschofenig, H. Securing the internet of things: A standardization perspective. IEEE Internet Things J. 2014, 1, 265–275. [Google Scholar] [CrossRef]
- Uludag, U.; Pankanti, S.; Prabhakar, S.; Jain, A.K. Biometric cryptosystems: Issues and challenges. Proc. IEEE 2004, 92, 948–960. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Platform | Deployment | Communications | Identification | Standards | Cloud |
|---|---|---|---|---|---|
| Rahmani et al. [30] | Hospital, Home | Bluetooth, Wi-Fi, 802.15.4/6LoWPAN | - | IEEE 1073 | Yes |
| Catarinucci et al. [31] | Hospital | 802.15.4/6LoWPAN | UHF-RFID | - | No |
| Cubo et al. [32] | Hospital, Home | 802.15.4 | NFC | - | Yes |
| Saponara et al. [33] | Nursing home, Home, Pharmacy | Bluetooth/BLE, Wi-Fi, 3G | - | HL7 CDA | Yes |
| Yang et al. [34] | Home | Wi-Fi, ZigBee | UHF RFID | - | Yes |
| Ghose et al. [35] | Home | Bluetooth, Wi-Fi, 3G | - | - | Yes |
| CRIP | Nursing home, Home | Bluetooth, Ethernet | Biometrics, NFC | Continua Alliance | Yes |
| ID | Description |
|---|---|
| UC1 | Health devices shall be seamlessly detected by the CRIP. |
| UC2 | Authenticated users shall be able to logon to the CAALHP via the CRIP. |
| UC3 | Health devices shall be defined by a Device Profile that is related to a CareStoreDeviceDriver in the CareStore Marketplace. |
| UC4 | CAALHP may communicate with health devices via the CRIP. |
| UC5 | Vital signs from health devices may be collected via the CRIP or the CAALHP. |
| UC6 | Read users’ credentials in order to be stored on the CareStore Marketplace. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, J.; Cabral, J.; Wagner, S.R.; Fischer Pedersen, C.; Ravelo, B.; Memon, M.; Mathiesen, M. An Open Platform for Seamless Sensor Support in Healthcare for the Internet of Things. Sensors 2016, 16, 2089. https://doi.org/10.3390/s16122089
Miranda J, Cabral J, Wagner SR, Fischer Pedersen C, Ravelo B, Memon M, Mathiesen M. An Open Platform for Seamless Sensor Support in Healthcare for the Internet of Things. Sensors. 2016; 16(12):2089. https://doi.org/10.3390/s16122089
Chicago/Turabian StyleMiranda, Jorge, Jorge Cabral, Stefan Rahr Wagner, Christian Fischer Pedersen, Blaise Ravelo, Mukhtiar Memon, and Morten Mathiesen. 2016. "An Open Platform for Seamless Sensor Support in Healthcare for the Internet of Things" Sensors 16, no. 12: 2089. https://doi.org/10.3390/s16122089